Demographics
and Practice Profile
Among
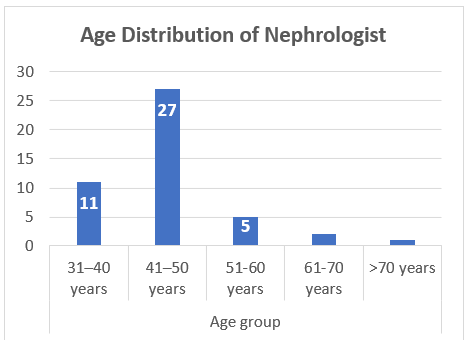
75 nephrologists practicing in Nepal, 46 responded (61.33%), comprising 89.13%
male (n=41) and 5 female doctors. 58.70% were in the age group 41-50 years (n=27).
About two-thirds have ≤10 years’ experience (n=32) and a DM Nephrology
qualification (n=26)—showing a relatively young, expanding workforce, 78.26%
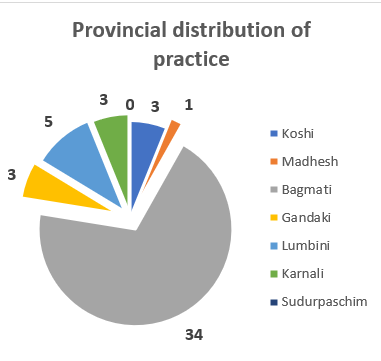
(n=36) practicing in either public or academic centers. A striking
centralization in Bagmati Province, 73.91% (n=34), and no Nephrologist working
in the Sudurpaschim Province indicating limited provincial presence.
76.09%
of the workforce works with typical small teams (≤3) per center, and many
specialists work across multiple sites to cover service gaps. While dialysis
access is expanding, the lack of transplant programs concentrates a heavy and
growing patient load onto a limited number of specialists.
There
is a significant waste of resources because many nephrologists who are
qualified to perform specialized procedures have stopped doing them. This issue
requires urgent attention.
Systemic
and Financial Challenges
Late
Patient Presentation is the most frequently cited "most significant
systemic challenge." Patients often present for the first time at CKD
Stage 4-5 or even when they need urgent dialysis, eliminating the option for PD
and optimal HD planning.
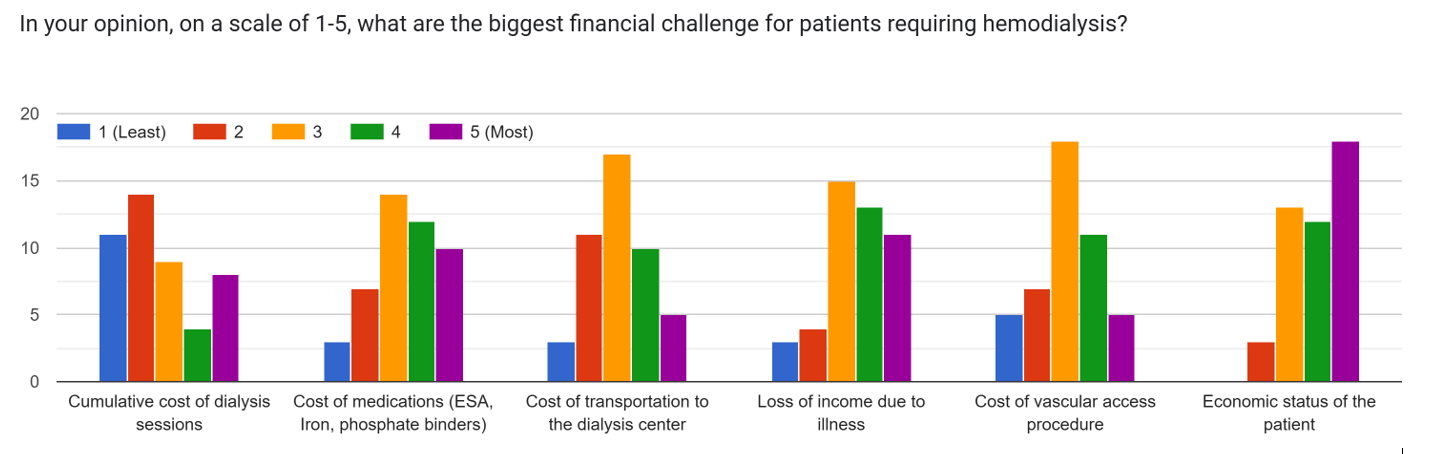
The
biggest financial challenges for patients are seen as the cumulative cost
of dialysis sessions and loss of income due to illness. The cost of
medications (like ESA and phosphate binders) is also a major factor.
Dialysis
Modalities and Access to Care
HD
is the overwhelming modality, with most respondents reporting >90% of
their maintenance dialysis patients on HD. PD utilization is minimal, often
<5%. The most common vascular access at HD initiation is
the Non-tunneled Central Venous Catheter, which is sub-optimal and
indicates a failure to create permanent access (Arteriovenous Fistula or AVF)
in a timely manner. This is a marker of late referral and/or lack of
pre-dialysis planning.
A
strong majority (82.6%, n=38) agree that patients are receiving inadequate
dialysis under the current government policy. Additionally, a large majority (91.3%,
n=42) agree with the statement: "The government policy regarding
HD/PD has definitely helped the patient financially, but the lack of scientific
basis and protocol has hampered Nephrologists to provide good standard
practice." This highlights a critical disconnect between
government support and clinical quality.
Barriers
to Peritoneal Dialysis (PD)
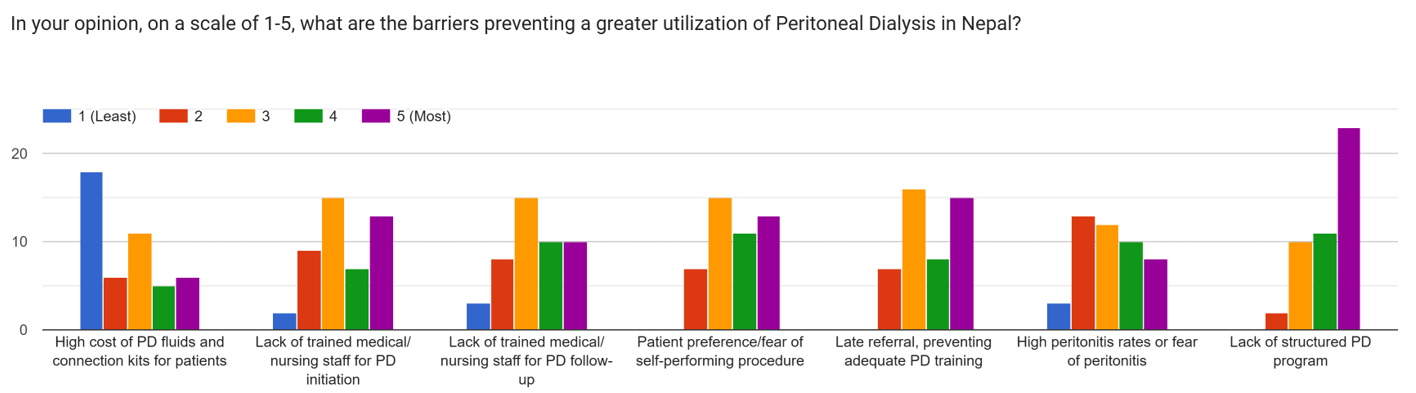
This
is a major focus of the survey. The primary barriers to PD, rated highly (4-5
on the scale), were:
· · Lack of Structured Programs: The absence of an
organized, hospital-wide PD program is a major systemic failure; 73.91%, n=34
· · Patient Fear/Preference: Fear of peritonitis and
reluctance to self-perform the procedure are significant patient-side barriers;
52.17%, n=24
· · Late Referral: Patients are referred too late to be
adequately trained for PD; 50%, n=23.
· Lack of Trained Staff: Both for initiation and
follow-up, a critical bottleneck; 43.48%, n=20.37%
(n=17) informed that there is no practice of pre-KRT counseling in their
institute, and an overwhelming 95.7% (n=44) would support the development of a
scientific PD program if given the opportunity.
Work
Satisfaction, Stress, and Burnout
Nephrologists
face an extremely heavy workload, typically working over 50 hours per week (54.34%,
n=25) on direct patient care, with many exceeding 70 hours (19.6%, n=9). They
are responsible for very large numbers of patients, often managing over 150
individuals for both chronic kidney disease and hemodialysis. This has led to
significant stress and burnout as a significant number of nephrologists report
frequent emotional exhaustion and burnout, with many experiencing these
feelings weekly or monthly. This high stress is further evidenced by a notable
tendency among some to view patients impersonally, a clear sign of professional
burnout.
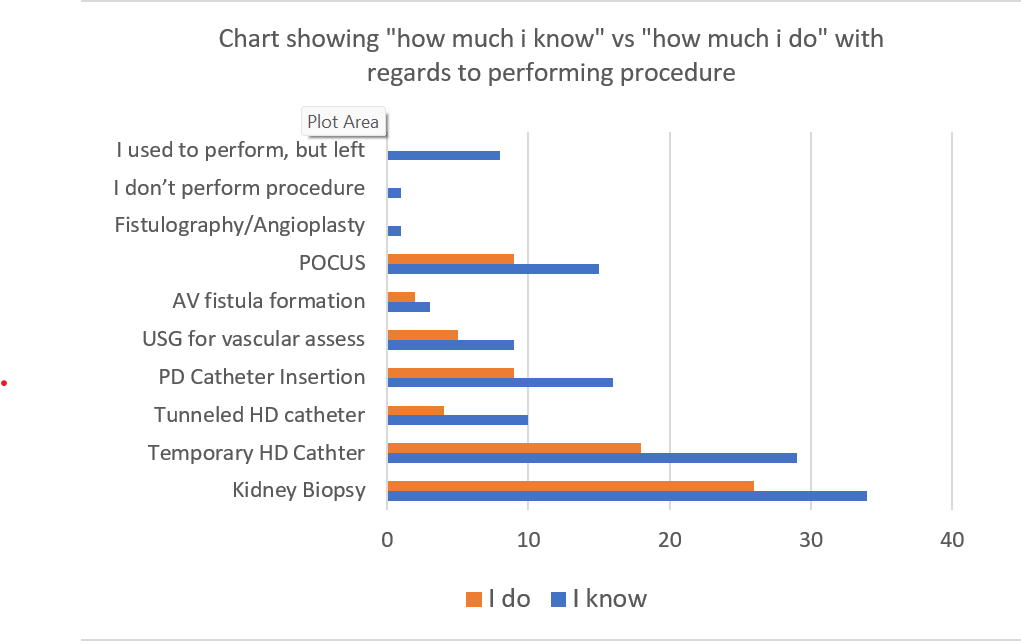
The data also reveals a concern in procedural skills among
nephrologists, creating a significant deficit. While a substantial number of
nephrologists are trained in various procedures, a far smaller subset performs
them routinely, as evidenced by the sharp decline from "can perform"
to "perform routinely": Kidney Biopsy (44 vs. 34), Temporary
Hemodialysis Catheter Insertion (39 vs. 25), Tunneled Hemodialysis Catheter
Insertion (13 vs. 6), and Peritoneal Dialysis Catheter Insertion (21 vs. 11).
This skills-practice gap is critically underscored by the fact that eleven
nephrologists have completely ceased performing procedures, and advanced skills
like AV Fistula formation have been entirely lost from active practice. This
leaves a profound gap between theoretical capability and on-the-ground service
delivery, posing a serious challenge to patient care and the development of
interventional nephrology in Nepal.
Nephrologists
seem to be motivated by the intellectual challenge of nephrology,
forming long-term relationships with patients, performing life-saving
procedures, and teaching.
Only 40 responses were available regarding the average salary; 55% (n=22) earned approximately. USD 1250 per month)
with only 17.5% (n=7) earning more than USD 2500 per month. The numerical
response could be misleading, but it’s a fact that the high workload and
immense responsibility are not being matched by perceived financial reward,
leading to overall career dissatisfaction.
Career
Plans and Future of the Specialty
This
is perhaps the most alarming finding, as a very large number of nephrologists
are considering significant changes in the next 5 years, including emigrating
to practice in another country (23.9%, n=11), pursuing further sub-specialty
training (often a precursor to emigration) (28.3%, n=13), reducing
clinical work hours (34.8%, n=16), or shifting to a non-clinical
role (administration, research, pharma) (13%, n=6). Only 18 (39.1%) nephrologists
were sure that they would continue the current practice in Nepal.
The
highest priority areas for development in Nepali nephrology were:
·
Improving
preventive nephrology and public awareness, 60.87% (n=28)
·
Strengthening and
expanding kidney transplant and peritoneal dialysis programs, 52.17% (n=24)
Developing
interventional nephrology programs, 47.83% (n=22)
