Case Reports
Case1
A 58-year-old male with ESRD secondary to autosomal dominant polycystic kidney
disease and CYP3A5 *3/*3 genotype received a deceased donor kidney transplant
(PRA 16%, anti-DR13 antibodies, KDPI 2%) with basiliximab induction. On
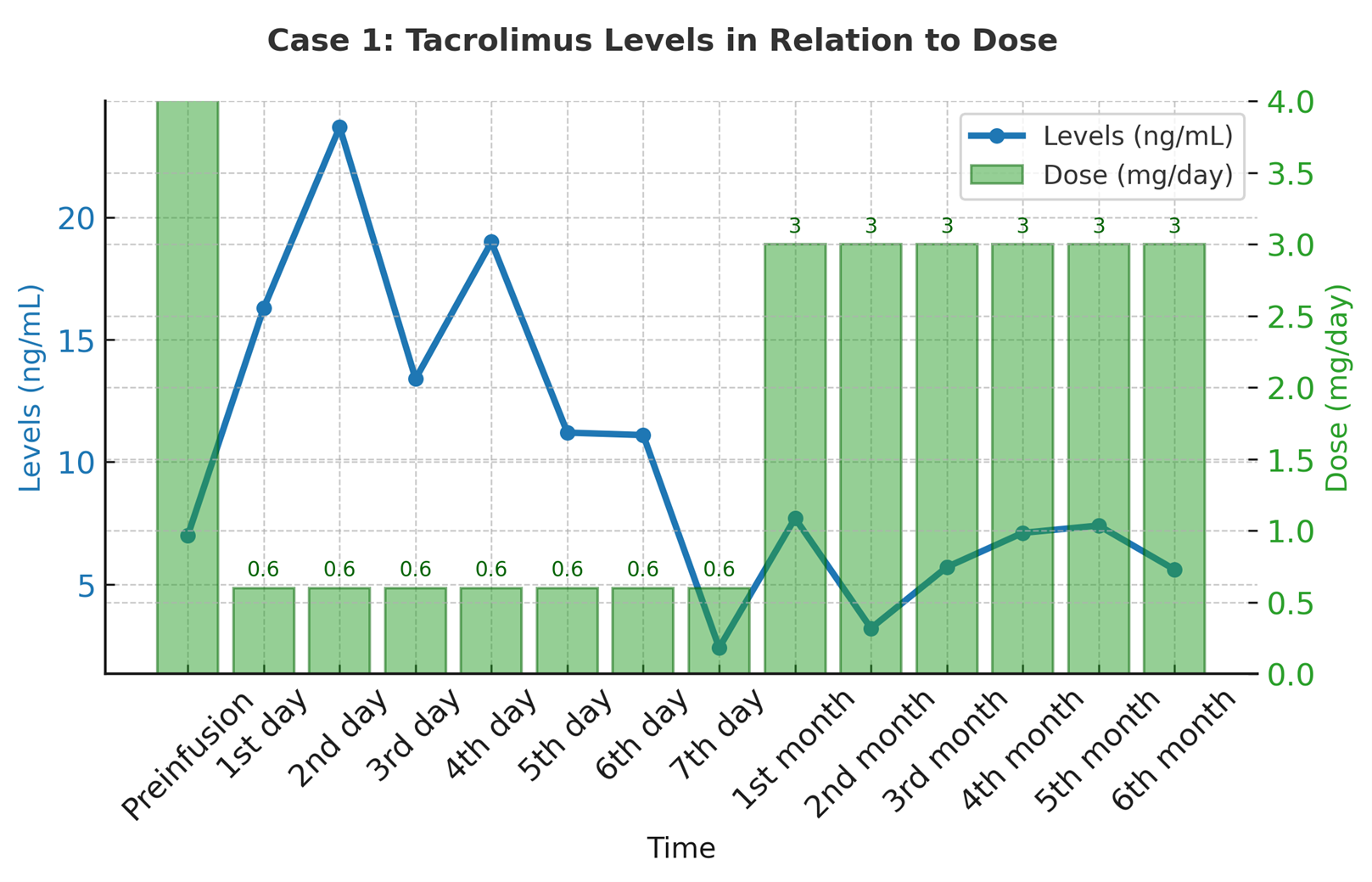
post-transplant day 15, IV tacrolimus (0.6 mg/24 h) was initiated due to
postoperative ileus following intestinal resection.
Figure 1: Tacrolimus serum
levels over 7 days. Despite constant IV dosing, trough levels fluctuated
between 11.2 and 23.7 ng/mL, reflecting slow metabolizer status.
Case2
A 56-year-old male with ESRD of unknown etiology, CYP3A5 *1/3 genotype,
received a deceased donor kidney transplant from expanded criteria donor (KDPI
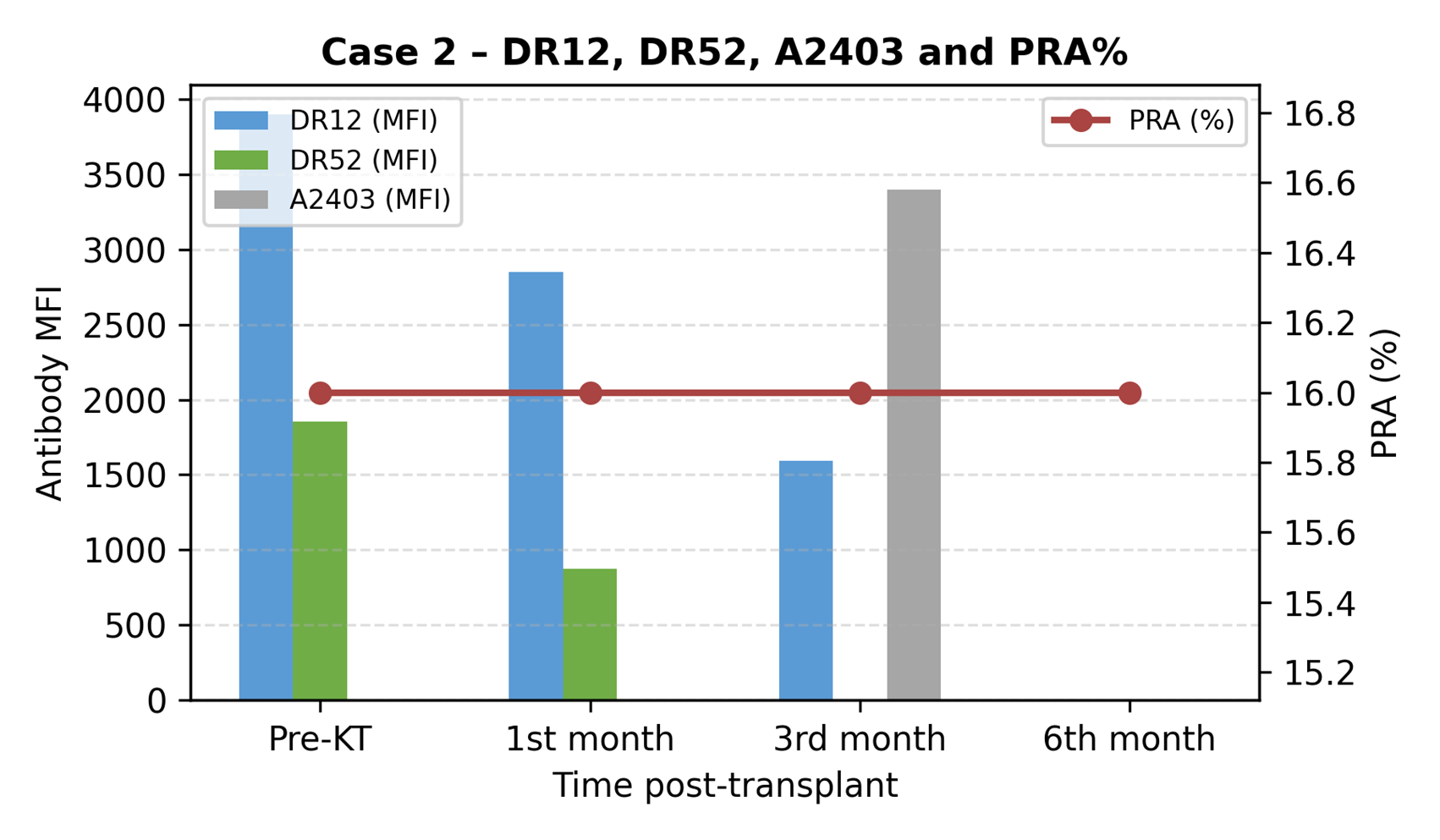
64%, PRA 16%, anti-DR12 and DR52 antibodies) with basiliximab induction. IV
tacrolimus (1.5–1.8 mg/24 h) was required for 9 days due to intestinal
perforation.
Figure 2: Tacrolimus serum levels over 9 days. Trough
levels remained stable between 5.0 and 5.6 ng/mL.
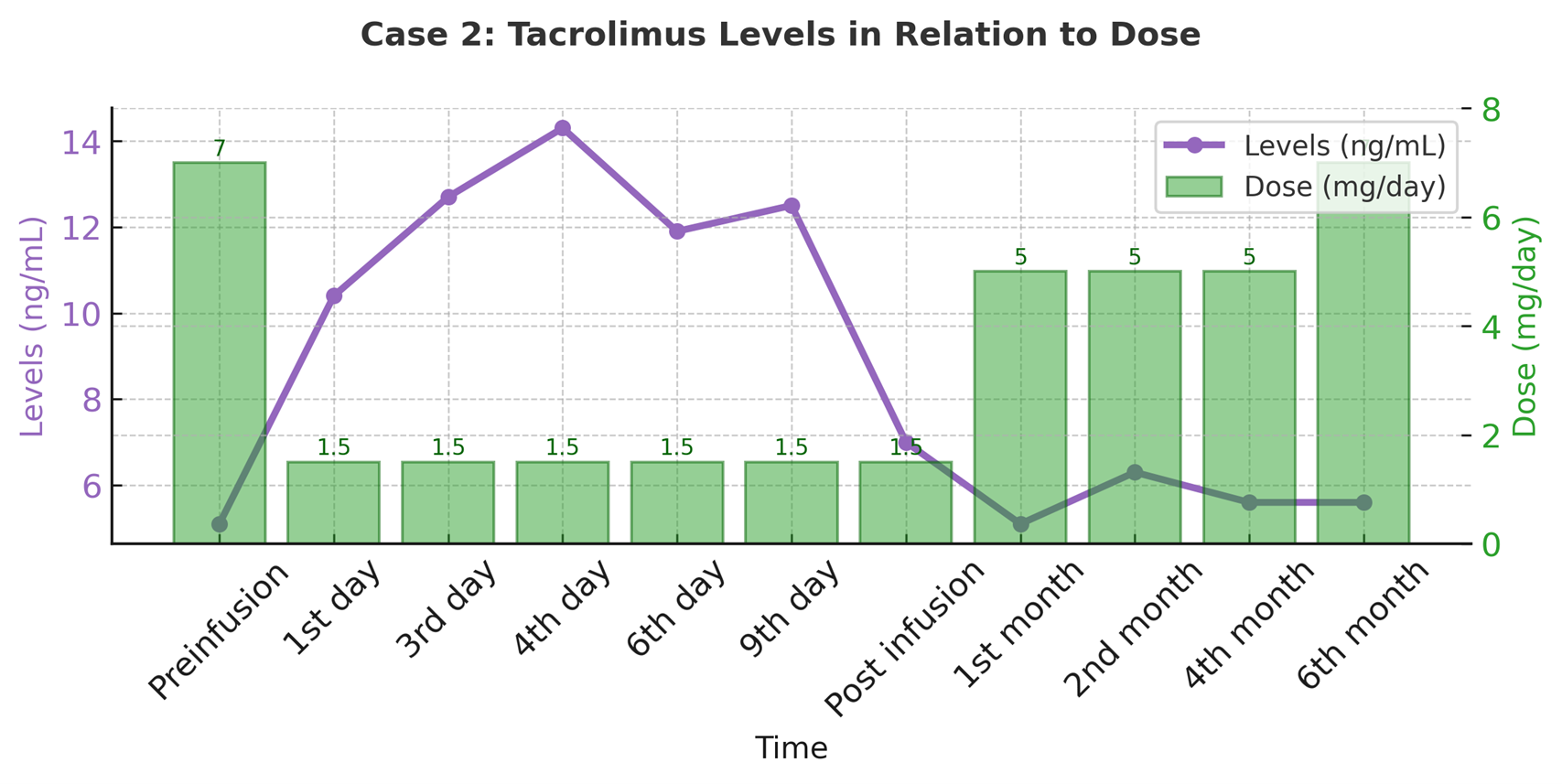
Figure 3: This figure shows the progression of serum
creatinine levels in two transplant cases over time, highlighting improvement
post-transplant.
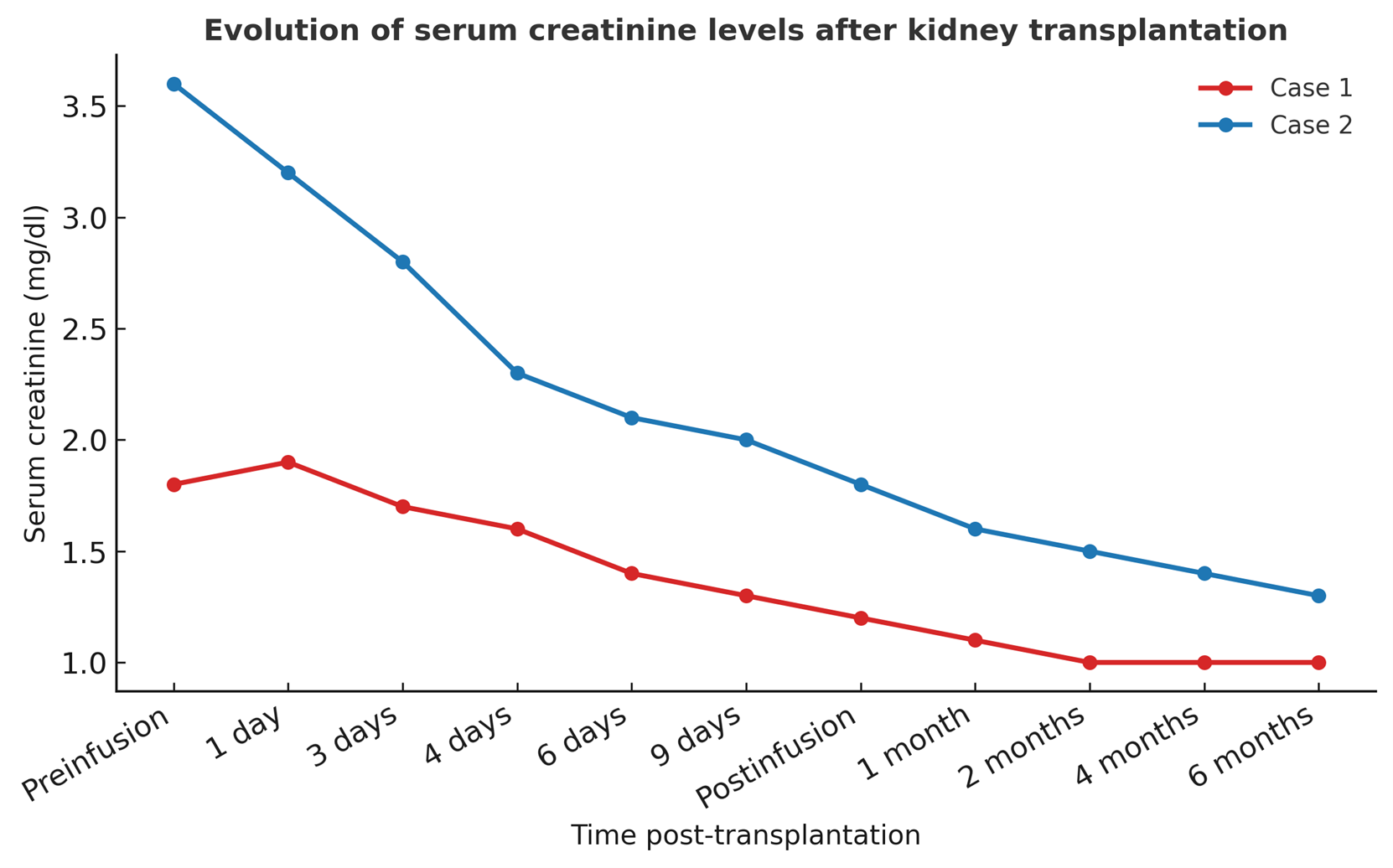
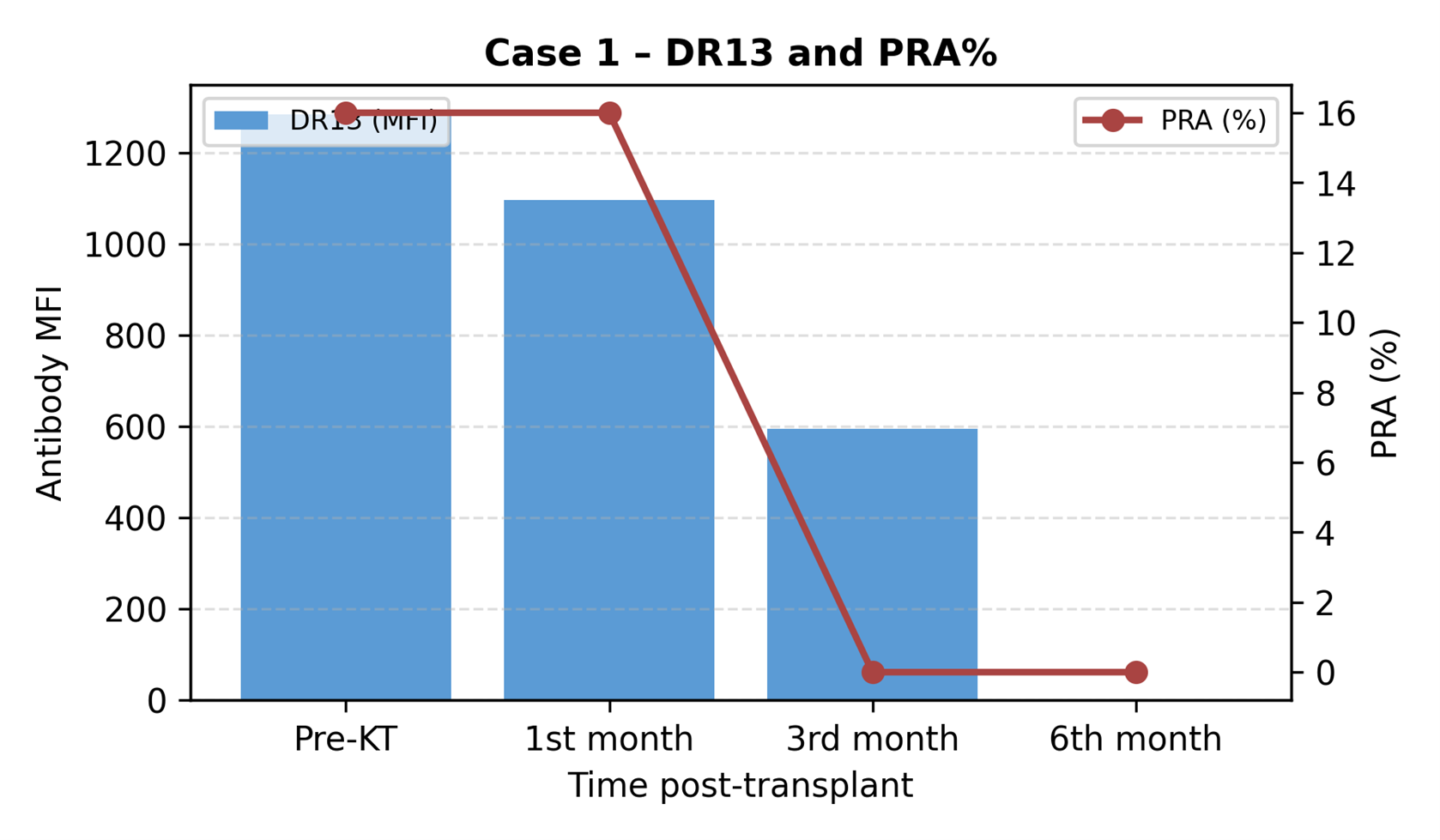
Figure 4: PRA and DSA evolution
for both cases over 6 months post-transplant.
Case 1: PRA and DR13 negativity at 6 months. Case 2:
reduction of DR12 and DR 52, but appearance of de novo anti-HLA, no ADEs.
Discussion
IV tacrolimus provides an
effective transitional route when oral administration is not feasible.
Continuous infusion over 24 hours, with individualized dosing based on body
weight and pharmacogenetic profile, allows for stable serum levels. CYP3A5
genotype strongly influences metabolism: slow metabolizers (*3/*3) show higher
variability (Case 1), whereas intermediate metabolizers (*1/*3) maintain
consistent trough levels (Case 2).
Ninguno de los pacientes
experimentó reacciones de hipersensibilidad, a pesar de la duración de la infusión
excedió los siete días recomendados. Esta constatación es pertinente, teniendo en cuenta que
los excipientes de tacrolimus intravenoso (aceite de ricino hidrogenado/polioxietileno)
puede inducir anafilaxia.
A pesar del difícil control de los niveles de tacrolimus en relación con el
dosis prescrita, la función del injerto fue favorable incluso para el caso 2, que presentó
retraso en la función del injerto y soporte de hemodiálisis requerido la primera semana
postrasplante, una condición esperada porque era un criterio ampliado
Trasplante, a los seis meses después del trasplante con creatinina delta de 0,5 mg/dl
entre ambos casos (1,0 mg/dl vs 1,5 mg/dl).
La monitorización de los virus BK y CMV es esencial para el seguimiento post-trasplante,
debido a la exposición a la inmunosupresión, lo que favorece el desarrollo de
infecciones oportunistas. Aunque la recomendación para el virus BK/JC y CMV
El seguimiento se realizará a los 1, 3, 6, 9 y 12 meses, en nuestro centro es
realizado mensualmente hasta el primer año después del trasplante, debido a la experiencia
que muchos pacientes desarrollan este tipo de infección incluso recibiendo profilaxis
(en el caso del CMV). El paciente del caso 1, que estuvo expuesto a dosis más bajas de
inmunosupresión, permaneció con BK/JC y CMV indetectables; Por el contrario, el
paciente en el caso 2 presentó <500 copias/ml de CMV sin requerir más
que la vigilancia
