CASE DESCRIPTION
The patient is a 30-year-old primigravid at 21 weeks old, initially presenting with easy fatigability, exertional dyspnea not associated with orthopnea, palpitation, cough or colds, visual disturbances, or unusual behavior. A few days later, the patient reported the onset of bilateral leg swelling initially up to the ankles. Initially assessed as physiologic edema of pregnancy and less likely of cardiac origin, the patient was discharged stable with close follow-up. Post-discharge, the bilateral leg edema persists, now with progression to the thighs, upper extremities, and face. Due to the progression of edema and eventual perceived uterine contractions, the patient was readmitted. Pertinent in her gestational history include an unremarkable Prenatal workup. Aside from a reactive Rubella IgG serology, Toxoplasmosis, Rubella IgM, and CMV serologies were nonreactive. Thyroid function tests were nonreactive. A Congenital Anomaly Scan done at 19 weeks of Gestation revealed findings consistent with Hydrops Fetalis, for which she was advised to undergo frequent ultrasound monitoring. Physical examination findings, including vital signs, cardiac and respiratory exam, were generally unremarkable, but of note are bilateral periorbital swellings and non-pitting edema of the bilateral dorsum, palms, and forearms. There was symmetric Grade 2 bilateral pitting edema of the lower extremities, reaching the thighs, still with appreciable 2+ pulses on bilateral dorsalis pedis arteries, without sensorimotor deficits, tenderness, gross skin lesions such as wounds, or skin discolorations.
The initial impression was Preeclampsia versus Pregnancy-Associated Cardiomyopathy. Review of laboratories done showed a urinalysis (dipstick value) protein value of 2+ and Urine Protein Creatinine ratio of 470 mg/g, which is considered significant proteinuria. Complete blood count revealed a hemoglobin of 8.7 mg/dL and a Hematocrit of 26.9 with a normal platelet count, consistent with delusional normocytic normochromic anemia without thrombocytopenia. Initially, creatinine was normal at 0.64 mg/dL with an estimated CKD-EPI 2021 eGFR of 119 mL/min/1.73m^2. Serum albumin was low at 3.11 mg/dL, and serum uric acid was elevated at 7.5 g/dL. Ancillaries seem to show an anomalous preeclampsia-like state. However, the patient did not have episodes of blood pressure of 140/90 mmHg or higher throughout her hospitalization; this prompts the consideration of another preeclampsia-like syndrome that could explain the anomalous progressive edema of our patient. Transthoracic 2D echocardiography and Venous Duplex Scan findings were also unremarkable, making heart failure or deep venous thrombosis less likely the etiology for the edema in this pregnant patient. With inconclusive results of ancillaries, but an anomalous preeclampsia-like picture, review of the obstetric workup done consistent with Hydrops fetalis helped ascertain the cause of the edema.
Repeat pelvic ultrasound at 21 weeks AOG showed the presence of scalp edema, ascites, and pleural effusion, fulfilling the diagnosis of a hydrops fetalis pregnancy. According to The Philippine Society of Maternal Fetal Medicine (2021), aside from the poor prognosis of hydrops fetalis pregnancies, there is a significant burden of hydrops fetalis pregnancies on the maternal side; mothers carrying hydropic fetuses are at risk of developing severe preeclampsia-like features collectively known as Mirror syndrome, a rare condition characterized by maternal edema that reflects or mirrors the edematous features of the baby affected by hydrops fetalis. The patient and the fetus fulfilled the three criteria required of mirror syndrome, specifically placentomegally defined as >5 cm after 21 weeks AOG, seen in the patient on Figure 1. AOG, hydrops fetalis as previously described, and clinical maternal edema, which was the chief complaint of the patient.
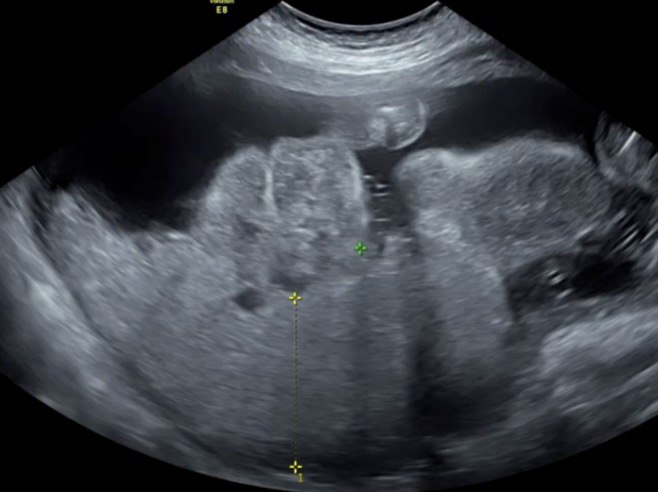
Figure 1. Pelvic Ultrasound of the patient at 21 weeks AOG showing placentomegaly. In January 2025, a placental thickness of 6.97 cm was observed, one of the criteria for mirror syndrome.
The patient’s dilutional anemia, hypoalbuminemia, hyperuricemia, and proteinuria without hypertensive episodes are also consistent with the clinical presentation of Mirror syndrome. Clinching the diagnosis of Mirror syndrome was vital as it is known to be associated with more extensive maternal morbidities, including a high likelihood of pulmonary edema, ICU admission, heart failure, and significant renal dysfunction.
Determination of the etiology of fetal hydrops is vital because addressing the specific etiology of the hydrops fetalis is known to lead to the resolution of mirror syndrome symptoms and improvement in perinatal outcome. However, the patient’s obstetric workup revealed no identifiable cause of hydrops fetalis. Anti-Ro and Anti-La antibodies, signifying autoimmune congenital heart block, were negative. Elevated Middle Cerebral Artery peak systolic velocity seen in ultrasonography is an accepted marker for fetal anemia, but the MCA PSV of the patient was normal, showing no evidence of Fetal anemia. Done as per the patient’s request, non-invasive prenatal testing, which identifies common chromosomal fetal pathologies, also tested negative. The inability to identify an etiology for the hydrops categorizes the fetal hydrops as idiopathic; hence, delivery was indicated due to deteriorating maternal status. As agreed upon by the healthcare team and the patient, the plan was to induce labor regardless of fetal outcome to resolve the clinical symptoms of the mother.
While undergoing cervical ripening, the patient developed progression of edema reaching up to the perineal area and labia, wth persistence of dilutional anemia as seen in Hemoglobin values as low as 8 mg/dL and Hematocrit as low as 24.6. The patient was referred for tapering urine output with no identifiable sources of fluid loss. On Day 6 of hospitalization, the patient had sudden oliguria with a urine output of 290 mL in 24 hours. POCUS done showed maximal expiration, IVC diameter of 1.1 cm with >50% collapsibility, suggesting reduced intravascular volume, likely suggesting Acute Kidney Injury, Prerenal from Decreased Effective Circulating Volume secondary to Third Spacing from Mirror Syndrome. Despite intravenous hydration with 5% Dextrose and 0.45% Sodium Chloride at rates as high as 120 ml/hr with 20% albumin infusion every 12 hours with Furosemide 20 mg intravenous bolus once a day, the patient still has oliguria as low as 394 ml in 24 hours (0.25 ml/kg/hour). Serum creatinine was noted to have elevated from 0.79 mg/dL to 1.09 mg/dL in 24 hours with a 2-hour post-furosemide urine output of 59 ml, indicating a high risk of progression to renal failure. Unresponsiveness to furosemide and oliguria persisted for another day until the spontaneous rupture of membranes occurred, prompting delivery. No adverse maternal intraoperative events, such as arrhythmias or hypotension, were noted. Despite the risk of postpartum hemorrhage in mirror syndrome, the estimated blood loss was only 117 mL.

Figure 2. Stillborn hydropic fetus delivered via partial breech extraction. The fetus was grossly edematous with low-set ears and a small nose.
A day after delivery, the bipedal edema persisted, but facial edema was noted to be regressing. The patient had improved urine output (1.150 ml/kg/hr) and was more responsive to diuretics with a post-furosemide output of 1425 ml. The Intravenous Fluid rate from 120 ml/hr was decreased to 10 ml/hr. After another day, there was significant regression of the pitting edema on the legs. On the day of discharge, the patient was seen comfortable, voiding freely, and still without hypertensive episodes. The facial edema and bilateral pitting edema resolved, and serum creatinine significantly decreased from 1.09 mg/dL to 0.70 mg/dL, indicating renal recovery post-delivery. Repeat urinalysis was unremarkable, and electrolytes were normal.
One month after discharge, the patient followed up with noted complete resolution of clinical edema. Repeat serum creatinine was 0.69 mg/dL, complete blood count was unremarkable with hemoglobin of 12.2 mg/dL and hematocrit of 36. Urinalysis showed the absence of proteinuria, showcasing the expected resolution of clinical and laboratory features of mirror syndrome post-delivery.
