Patient K. is a girl
with albinism, 14 years
old, from
a medical history of the disease: she has been suffering from congenital nephrotic
syndrome since 2011.
On December
11, 2015,
a kidney
transplant from a cadaverous
donor was performed.
In September
2021, the
patient had: chronic
graft disease,
5 -
terminal stage.
On
09.14.2021, a Tenkoff peritoneal dialysis catheter
was implanted. PD was
started on 09.15.2021.
On 04.20.2023, an operation
was performed – a lumbotomy on the right. Transplantectomy.
Nephroterectomy of the native kidney
on the right. The patient
had symptomatic
arterial hypertension of 2-3 degrees
against the background of PD and
non-compliance:
160-170/125-130 mmHg.
The patient
was hospitalized in the UMC
Hospital OND from 02.21-31.03.2024:
03.05.2024 surgery was performed to eliminate a hernia
of the anterior abdominal wall
with dissection.
The patient was re-hospitalized in the
UMC Hospital on 04.01.2024: Clinical problems
at admission:
- malignant
course of symptomatic arterial
hypertension on the background
of combined arterial hypertension
- anemia
of moderate severity Hb
88g/l
-
thrombocytopenia 66-144 thousand.
-
inability to perform HRT:
PD (the
patient has a high
risk of
leakage of dialysis fluid
through postoperative wounds, there
is a risk of recurrence
of ventral hernia, it was decided to refrain
from PD for 14
days), continued HRT:
HD
-
coagulopathy has an unclear
origin, and therefore hemodialysis
sessions are performed without the use
of heparin.
On 04.05.2024, at
13:15, the patient's
condition during examination
was severe in dynamics
with deterioration,
unstable, due to arterial
hypertension of 210/100 mmHg,
severe pain syndrome,
noticeably cold sticky
sweat, crying, screaming.
At the same time, the heart rate-68-90/ one minute, BH-24-26/ for a minute, SpO2
is 100%. 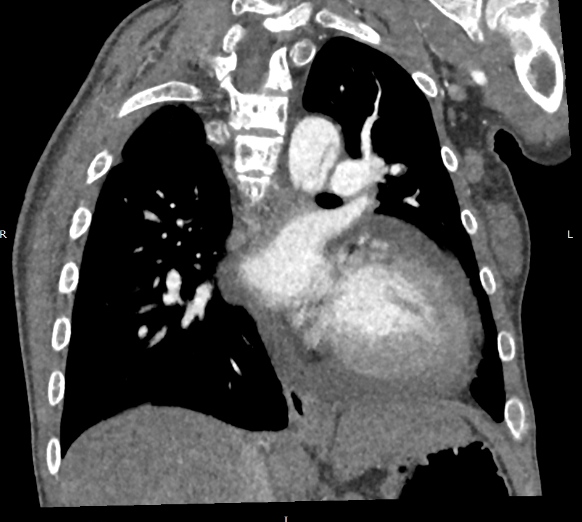 on 04.05.2024: signs
of a dissecting aortic aneurysm
(
on 04.05.2024: signs
of a dissecting aortic aneurysm
(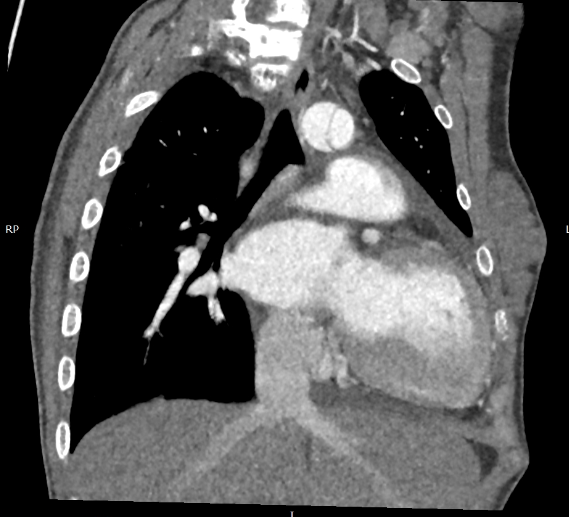
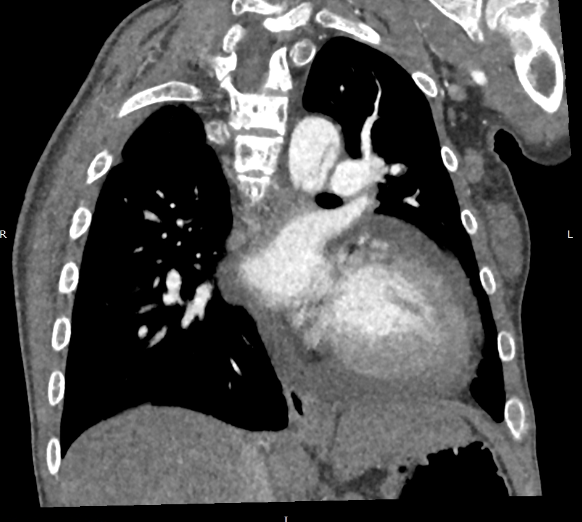 ) with
spread to the mouth
of the left subclavian artery,
the mouth of the right common
iliac artery and up
to the bifurcation of the left common
iliac artery
(with subtotal
thrombosis of the lumen of the vessel of the left common
iliac artery,
thrombosis spreads to
proximal segment of the left internal
iliac artery
) with
spread to the mouth
of the left subclavian artery,
the mouth of the right common
iliac artery and up
to the bifurcation of the left common
iliac artery
(with subtotal
thrombosis of the lumen of the vessel of the left common
iliac artery,
thrombosis spreads to
proximal segment of the left internal
iliac artery );
hemodynamically significant stenoses
of the LAD and the mouth
of the superior mesenteric artery
on the background of atherosclerotic plaques; pericarditis;
left ventricular
myocardial hypertrophy; multiple small-focal seals
of both lungs (to
differentiate with hypersensitive
pneumonitis and fungal
lesions); mediastinal, axillary, retroperitoneal,
inguinal lymphadenopathy. She was consulted
by an angiosurgeon: Acute dissection
of the aorta in the thoracic
region, DeBayko type 1.
Recommended: CT scan of the abdominal aorta,
iliac arteries
with contrast
with further
consultation with a cardiac surgeon. She was consulted by a cardiac surgeon on
04.05.2024. She was diagnosed with acute exfoliating
aneurysm of the ascending thoracic
aorta, aortic arch,
descending aorta, SNFC
IV. 04.05.2024
19:40-19:50: A consultation
was held, taking into account clinical and anamnestic, laboratory
and instrumental data, it was decided to carry
out surgical intervention in the following volume: "Supracoronary
prosthetics of the ascending aorta
with a vascular prosthesis."
The risk on the basic
Aristotle scale is 11
points (mortality is 10-20%, the risk
of complications, the duration of stay
in the ICU is 1-2
weeks, the complexity is significant). The expanded Aristotle
scale is 16.0 (+1
for renal
failure, +3 points
for chronic kidney failure requiring regular dialysis,
+1 for
acquired coagulation disorder),
(mortality of more than 20%,
risk of complications, duration of ICU
stay of more than 2
weeks, increased complexity).
Operation 04/05/2024 20:50h-4:00h:
Supracoronary prosthetics of the ascending aorta
with a vascular prosthesis "Vascutek
– 24
mm" in conditions
of artificial circulation, deep hypothermia
and circulatory
arrest. After the operational
period, there was:
1) signs
of ongoing active bleeding,
2) acute
cardiovascular insufficiency: unstable hemodynamics,
arterial hypotension. 04.07.2024, the patient's condition
is critical with progressive
deterioration 03:00 against the background
of progressive heart failure,
increased hypotension, cardiac arrest occurred, 03:30
biological death was pronounced.
);
hemodynamically significant stenoses
of the LAD and the mouth
of the superior mesenteric artery
on the background of atherosclerotic plaques; pericarditis;
left ventricular
myocardial hypertrophy; multiple small-focal seals
of both lungs (to
differentiate with hypersensitive
pneumonitis and fungal
lesions); mediastinal, axillary, retroperitoneal,
inguinal lymphadenopathy. She was consulted
by an angiosurgeon: Acute dissection
of the aorta in the thoracic
region, DeBayko type 1.
Recommended: CT scan of the abdominal aorta,
iliac arteries
with contrast
with further
consultation with a cardiac surgeon. She was consulted by a cardiac surgeon on
04.05.2024. She was diagnosed with acute exfoliating
aneurysm of the ascending thoracic
aorta, aortic arch,
descending aorta, SNFC
IV. 04.05.2024
19:40-19:50: A consultation
was held, taking into account clinical and anamnestic, laboratory
and instrumental data, it was decided to carry
out surgical intervention in the following volume: "Supracoronary
prosthetics of the ascending aorta
with a vascular prosthesis."
The risk on the basic
Aristotle scale is 11
points (mortality is 10-20%, the risk
of complications, the duration of stay
in the ICU is 1-2
weeks, the complexity is significant). The expanded Aristotle
scale is 16.0 (+1
for renal
failure, +3 points
for chronic kidney failure requiring regular dialysis,
+1 for
acquired coagulation disorder),
(mortality of more than 20%,
risk of complications, duration of ICU
stay of more than 2
weeks, increased complexity).
Operation 04/05/2024 20:50h-4:00h:
Supracoronary prosthetics of the ascending aorta
with a vascular prosthesis "Vascutek
– 24
mm" in conditions
of artificial circulation, deep hypothermia
and circulatory
arrest. After the operational
period, there was:
1) signs
of ongoing active bleeding,
2) acute
cardiovascular insufficiency: unstable hemodynamics,
arterial hypotension. 04.07.2024, the patient's condition
is critical with progressive
deterioration 03:00 against the background
of progressive heart failure,
increased hypotension, cardiac arrest occurred, 03:30
biological death was pronounced.
