During study period, 520 adult patients were admitted;
of them, 401 were excluded (235 had no AKI; 96 had AKI, but died within 7 days
of AKI, 58 had pre-existing renal disease; 12 were pregnant). A total of 119 patients were included in the
present study, median age of 38 years (29-52), 68.9% were male, predominantly
(82.4%) with medical illness preceding ICU admission. Up to 85% and 82% of
these patients were on mechanical ventilatory and vasopressor support
respectively. Mortality in the study cohort in ICU was 42.9% (n=51). MAKE 90
outcome occurred in 43.7 % (n=52) of the study population. Among patients with
MAKE 90 outcome, plasma NGAL: 4538 (3896-4736) versus 3979 (2146-4654); p=0.05, urine NGAL: 1451
(1128-1925) versus 1124 (1004-1411); p= 0.02, plasma KIM1 levels : 499 (148-1089) versus 240 (55.6-326); p=0.03, were
significantly higher on day of AKD onset (day7), while plasma NGAL: 4536 (3456-4878) versus 1604 (1110-2075) ; p=0.02, and plasma KIM:1756 (486-826) versus 159 (117-200) ;p=0.02, were
significantly higher at ICU discharge compared to patients who did not achieve
MAKE 90 outcome. Also, plasma and urinary biomarkers at day 90 (n=25) (all in
patients with serum creatinine resolution), remained well above accepted
cut-off values for plasma NGAL, urine NGAL and plasma KIM-1 among 44%, 64% and 96%
of study participants, respectively.
Table
1: Baseline
characteristics of the study participants(n=119)
|
Baseline
Characteristics (n=119)
|
Median
(IQR)/number (%)
|
|
Age (years)
|
38 (29-52)
|
|
Male
|
82 (68.9)
|
|
Type of admission
(medical)
|
98 (82.4)
|
|
No. on mechanical
ventilator
|
102 (85)
|
|
No. on vasopressor
supports
|
98 (82)
|
|
Charlson co-morbidity
index
|
1 (0-2)
|
|
Vasopressor days
|
5 (3-8)
|
|
Mechanical ventilation
days
|
8 (6-12)
|
|
APACHE_II
|
16 (11-21)
|
|
Admission SOFA
|
9 (6-12)
|
|
AKI stage at ICU admission
(0/1/2/3)
|
14/31/29/45
|
|
Creatinine (mg/dL) at ICU
admission (mg/dL)
|
1.9 (1.21-3.45)
|
Abbreviations
used: APACHE: acute physiology and chronic
health evaluation; SOFA: sequential organ failure score ; AKI: acute
kidney injury; ICU: intensive care unit
Table
2: Outcome parameters of the study
participants (n=119)
|
Outcome
parameters (n=119)
|
Median
(IQR)/number (%)
|
|
Day of diagnosis of AKI
during ICU stay
|
5 (3-6)
|
|
LOS_ICU (days)
|
12 (7-15)
|
|
LOS_hosp (days)
|
15 (12-21)
|
|
28-day mortality
|
51 (42.9)
|
|
AKD at discharge (n=68)
AKD stage (0/1/2/3)
RRT dependent
|
57/2/4/5
6
|
|
Creatinine (mg/dL) at ICU
discharge (n=68)
|
0.79 (0.57-1.0)
|
|
AKD at 90 days (n=29)
Stage 0/1/2/3
RRT dependent
|
28/0/0/1
01
|
Abbreviations
used: LOS_ICU: length of stay intensive care
unit; LOS_hosp: Length of stay hospital; AKD: acute kidney disease; RRT: renal
replacement therapy
Table
3: Biomarker levels in study participants at
the diagnosis of AKD, ICU discharge in survivors and 90day post AKI diagnosis.
(#: lost to follow up: 43)
|
Biomarker
|
Median
(IQR)
|
|
At
AKD diagnosis (n=119)
|
|
P-NGAL
(ng/ml)
|
4099
(3449-4701)
|
|
U-NGAL
(ng/mg of UCr) (n=106)
|
1263
(1038-1796)
|
|
P-KIM-1
(ng/ml)
|
297
(111-881)
|
|
U-KIM-1
(ng/ml) (n=106)
|
883
(462-1533)
|
|
At
ICU discharge (n= 68)
|
|
P-NGAL
(ng/ml)
|
1412
(1113-1843)
|
|
U-NGAL(ng/ml)
(n=63)
|
658
(178-897)
|
|
P-KIM-1
(ng/ml)
|
121
(45-186)
|
|
U-KIM-1
(ng/mg of Ucr) (n=63)
|
297
(174- 297)
|
|
At
90 days post AKI diagnosis (n=25#)
|
|
|
P-NGAL(ng/ml)
|
167
(114-367)
|
|
U-NGAL(ng/ml)
|
117
(47-299)
|
|
P-KIM-1
(ng/ml)
|
56
(44-73)
|
|
U-KIM-1(ng/mg
of Ucr)
|
56
(43-77)
|
Abbreviations
used: P-NGAL: Plasma-Neutrophil-Gelatinase-Associated-Lipocalin (NGAL),
P-KIM-1: plasma kidney-injury molecule-1 (KIM-1); U-NGAL: Urine- Neutrophil-Gelatinase-Associated-Lipocalin
(NGAL),U-KIM-1: Urine kidney-injury molecule-1 (KIM-1); AKD: acute kidney
disease; AKI: acute kidney injury.
Table 4: Comparison
of plasma and urinary biomarkers in patients with and without MAKE 90 outcome
|
|
With
MAKE 90 (n=52)
|
Without
MAKE 90(n=34)
|
p-value
|
|
At
the onset of AKD
|
|
P-NGAL
(ng/ml)
|
4538
(3896-4736)
|
3979
(2146-4654)
|
0.05
|
|
U-NGAL
(ng/mg of UCr)
|
1451
(1128-1925)
|
1124
(1004-1411)
|
0.02
|
|
P-KIM (ng/ml)
|
499 (148-1089)
|
240 (55.6-326)
|
0.03
|
|
U-KIM(ng/mg
of UCr)
|
789(333-1364)
|
895 (545-1860)
|
0.45
|
|
At
ICU discharge
|
|
P-NGAL (ng/ml)
|
4536 (3456-4878)
|
1604 (1110-2075)
|
0.02
|
|
U-NGAL
(ng/mg of UCr)
|
-
|
647 (135-864)
|
0.48
|
|
P-KIM (ng/ml)
|
756 (486-826)
|
159 (117-200)
|
0.02
|
|
U-KIM(ng/mg
of UCr)
|
-
|
174 (135-385)
|
0.97
|
|
At
day 90
|
|
P-NGAL
(ng/ml)
|
261
|
163
(114-357)
|
0.59
|
|
U-NGAL
(ng/mg of UCr)
|
-
|
132 (46-331)
|
-
|
|
P-KIM (ng/ml)
|
56
|
56
(44.3-75.4)
|
1.0
|
|
U-KIM(ng/mg
of UCr)
|
-
|
57 (42-77.6)
|
-
|
Abbreviations
used: Abbreviations used: P-NGAL: Plasma-Neutrophil-Gelatinase-Associated-Lipocalin
(NGAL), P-KIM-1: plasma kidney-injury molecule-1
(KIM-1); U-NGAL: Urine- Neutrophil-Gelatinase-Associated-Lipocalin (NGAL),U-KIM-1:
Urine kidney-injury molecule-1 (KIM-1); AKD: acute kidney disease; AKI:
acute kidney injury.
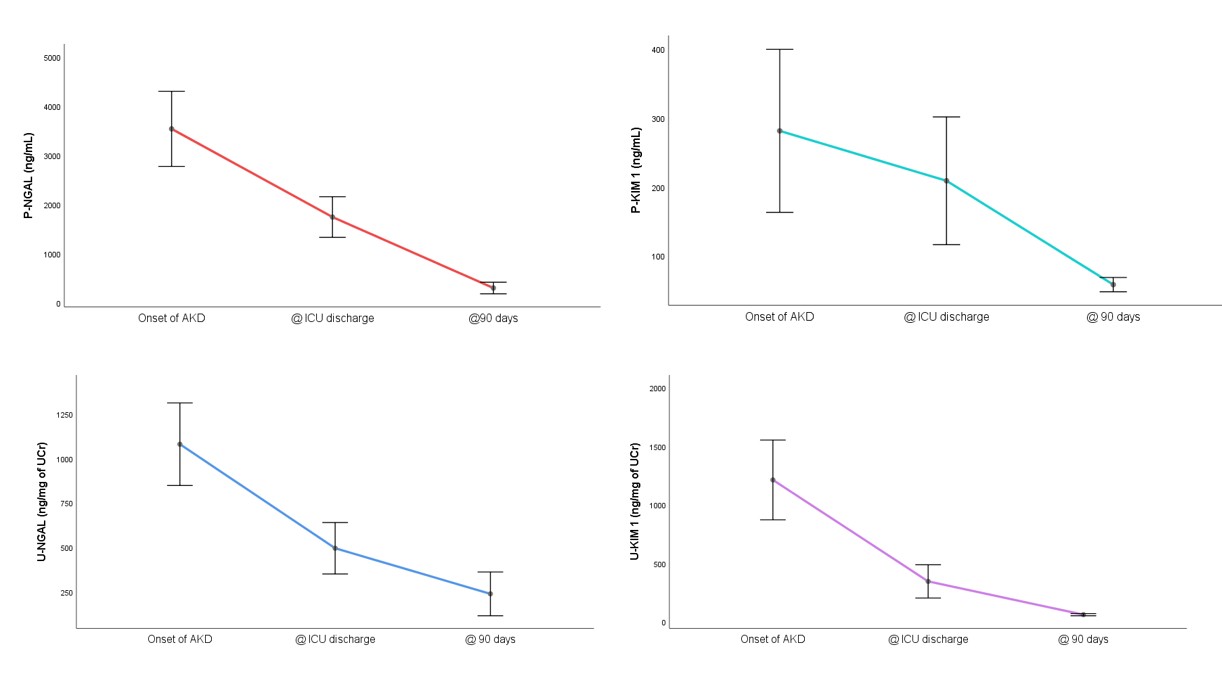
Figure 1: Progression
of biomarkers in patients with AKD at different time points.