A total of 141 procedures in 27 patients were analyzed. Of the patients included, 15 (55.5%) were women and 12 (44.4%) were men. The mean age was 51 years old, with an age predominance between 40 and 60 years old.
The distribution of indications for DFPP according to the ASFA recommendations were as follows (Chart 1):
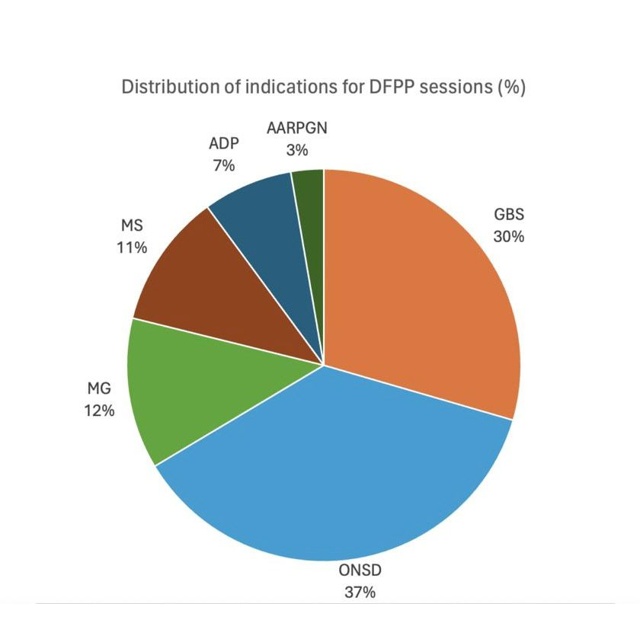
Category I:
*Guillain-Barré syndrome (GBS) (29,6%)
*Myasthenia gravis (MG) (12,5%)
*Acute demyelinating polyneuropathy (ADP) (7,4%)
*ANCA-associated rapidly progressive glomerulonephritis (AARPGN) (2.7%)
Category II:
*Multiple sclerosis (MS) (11,1%)
*Optic neuritis spectrum disorders (ONSD) (37%)
The reported complications following the procedure were:
*Central line-associated bloodstream infections (25,9%)
*Low serum fibrinogen < 100 mg/dL (9,2%)
*Clinical hypertension (4,2%)
*Deep vein thrombosis (2,7%)
*Thoracic duct laceration (2,7%)
*Air embolism 2,7%)
*Hypotension-induced seizure (2,7%)
*Central line hemorrhage (2,7%)
Clinical response was evaluated by a certified clinical neurologist according to subjective criteria. There was complete response in 33.3% of patients, partial response in 62.9% of patients, and no response in 2.7% of patients. The overall in-hospital mortality during the study period was 0%.
