1.Baseline Characteristics
A total of 122 patients were enrolled (54.9% male). The median age was 40.5 years, Scr was 97.0 μmol/L, and proteinuria was 1.2 g. Pathological data (Oxford MEST-C classification) were available for 77 patients. Budesonide was given as monotherapy (n=82, 67.2%) or combination therapy (n=40, 32.8%) (Table 1).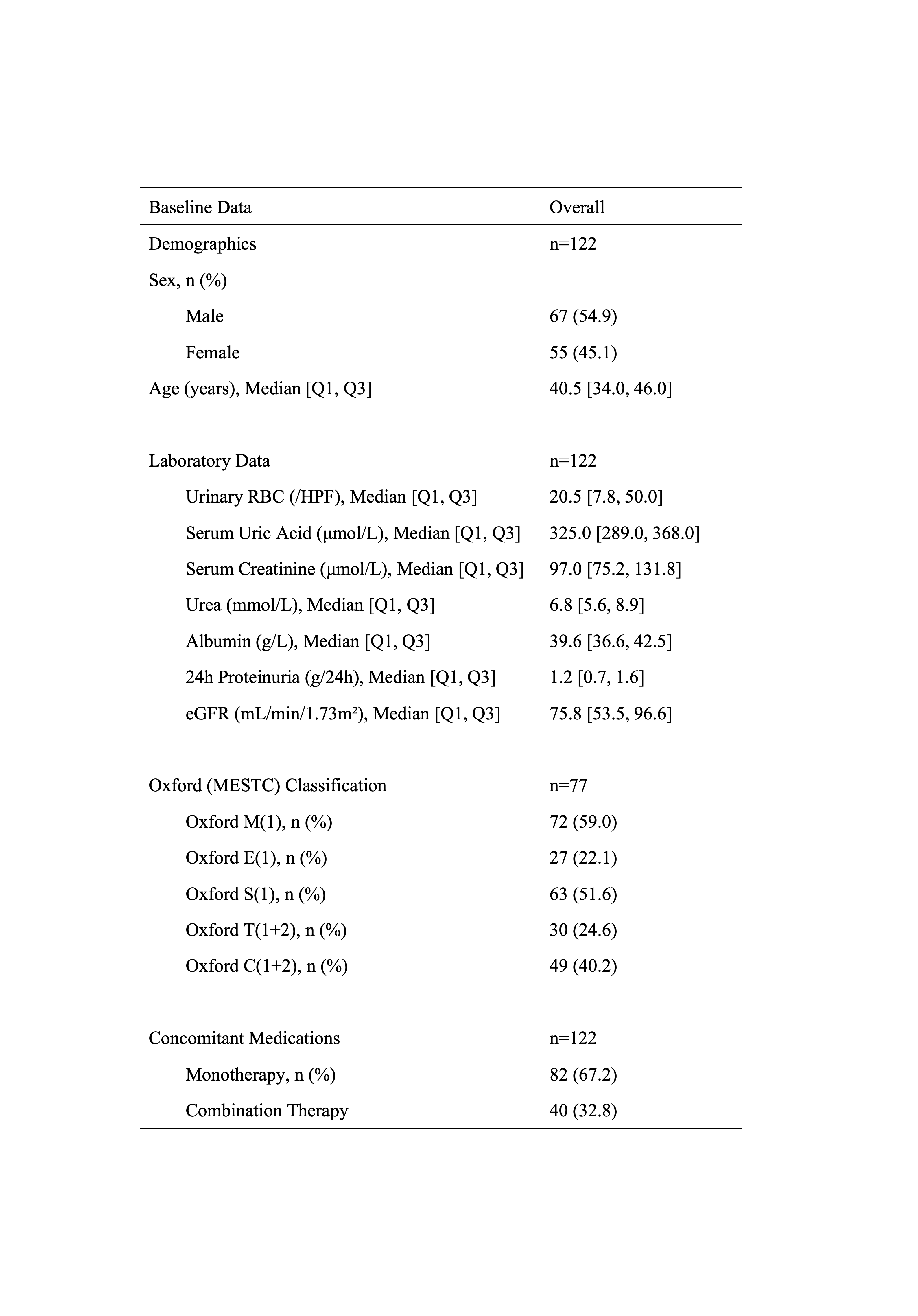
2. Efficacy Analysis
2.1 Overall Efficacy
Significant clinical improvements were observed over 6 months in the overall cohort.
Proteinuria and hematuria showed median reductions of 42% and 59.4%, respectively, at 6 months (p < 0.05 vs. baseline). Renal function remained stable, with a median eGFR increase of 5.8%. The ORR reached 40.3% at 6 months(Figure 1).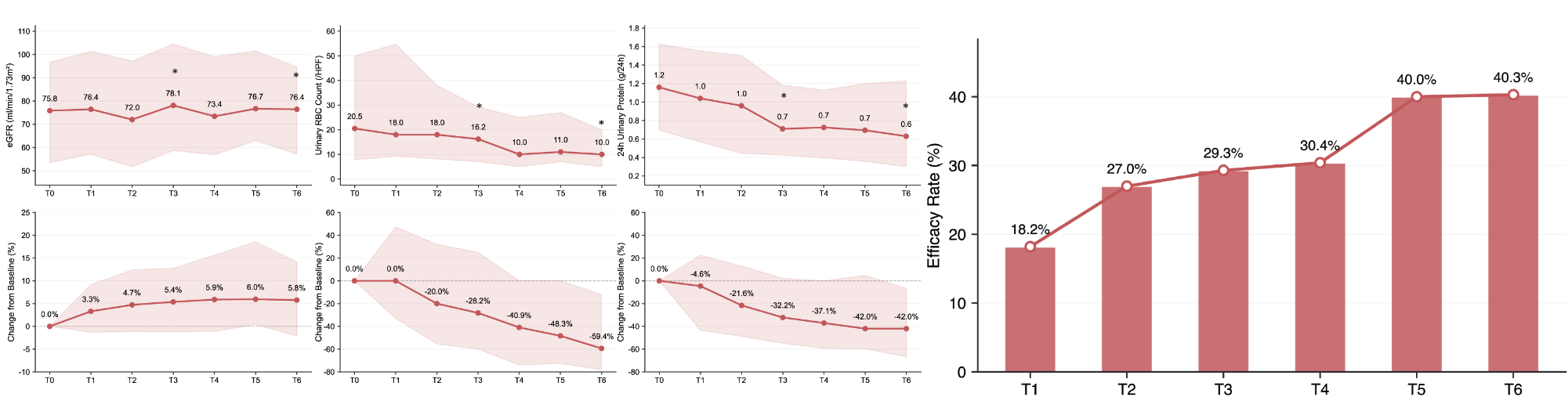
2.2.1 Subgroup Analysis by Baseline Proteinuria
Proteinuria reduction was significantly greater in the high-proteinuria group (≥1 g/d, n=75) than in the low-proteinuria group. However, the ORR at the 6th month was numerically higher in the low-proteinuria group (<1 g/d, n=47) with no significant difference. Both subgroups showed comparable improvements in eGFR. Additionally, they showed significant reductions in uRBC from baseline, with comparable percent changes(Figure 2).
2.2.2 Subgroup Analysis by Baseline eGFR
The low eGFR group (<60, n=42) showed significant improvement in renal function at 6 months (median increase: 15.2%), while the high eGFR group (≥60, n=80) remained stable. Both subgroups showed significant reductions in proteinuria and uRBC from baseline, with no significant between-group differences in percent reductions or ORR at the 6th month(Figure 3).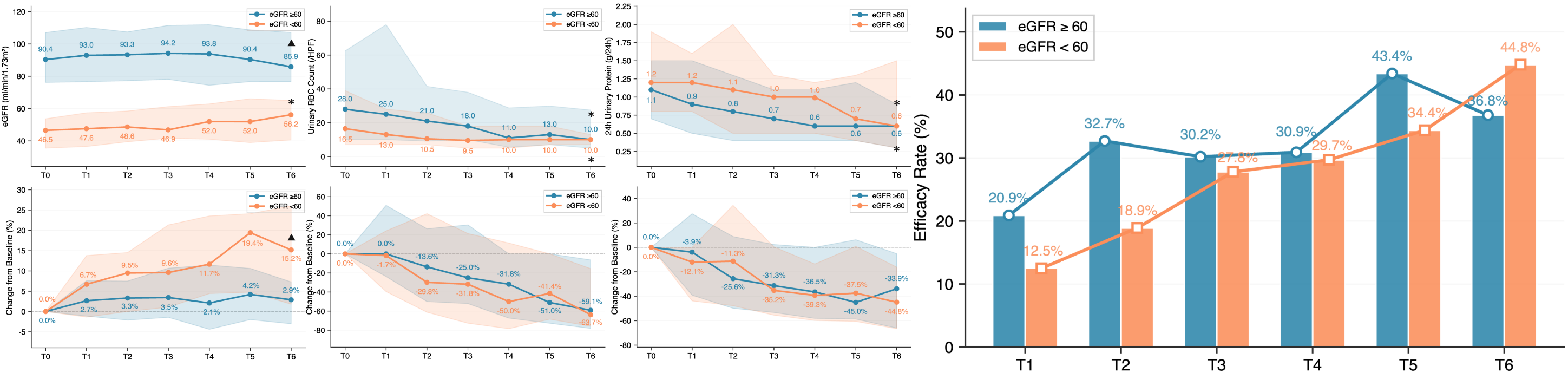
2.2.3 Subgroup Analysis by Prior Treatment Status
Both treatment-naive (n=101) and re-treatment patients (n=21) maintained stable renal function. Proteinuria and uRBC decreased significantly from baseline in both subgroups, with significantly greater reductions in treatment-naive patients(Figure 4).
2.2.4 Subgroup Analysis by Time from Biopsy
Proteinuria and hematuria decreased significantly from baseline in both subgroups. The early treatment group (biopsy <4 years, n=50) demonstrated significantly greater percent reductions in proteinuria and uRBC, as well as higher ORR, compared to the delayed treatment group (≥4 years, n=72). No significant between-group difference was observed in eGFR changes at the 6th month(Figure 5).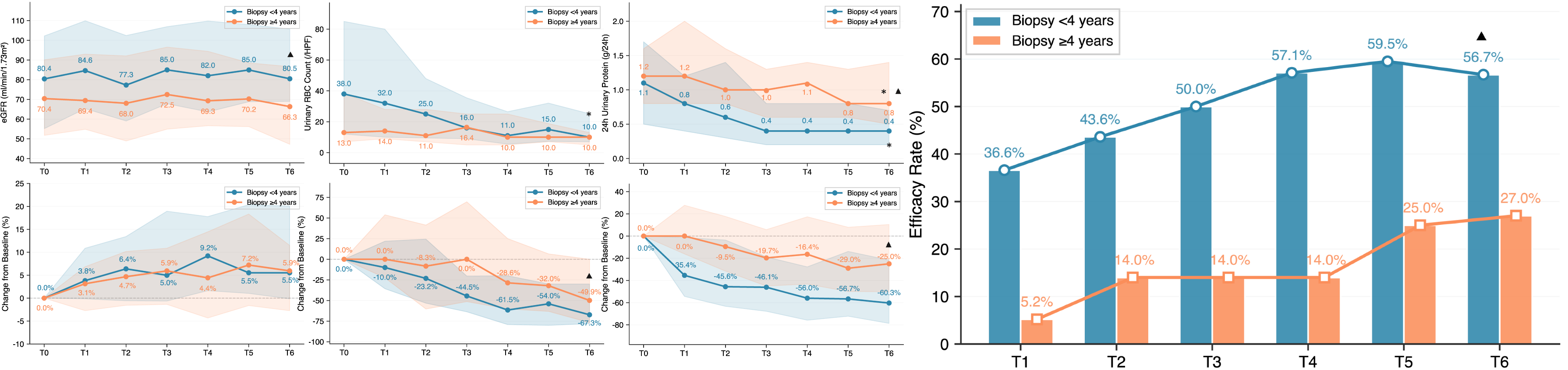
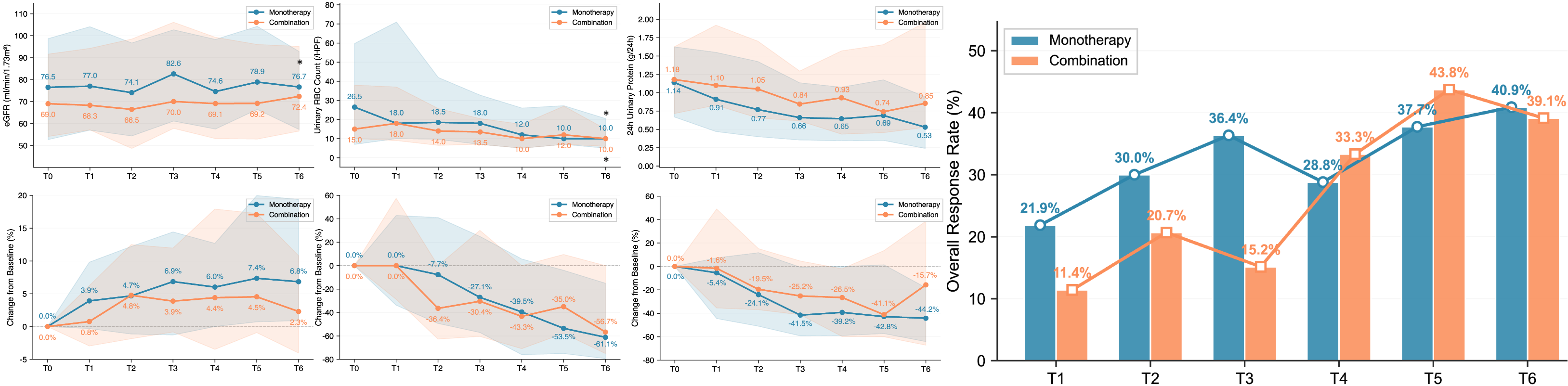
2.2.5 Subgroup Analysis by Treatment Regimen
Compared between monotherapy (n=82) and combination therapy (n=40) groups there were no significant differences in terms of proteinuria and uRBC relief, eGFR changes or ORR(Figure 6).