We describe
our experience of growing a sustainable PD program and revenues through a
medical collaboration model between the PD team consisting of nephrologists,
nurses, dieticians, pharmacists, social workers, physical therapists,
psychologists, using teamwork approach, and PCPs from 2005 to 2024 at Kokura
Memorial Hospital (KMH). Up to 2004, there were no PD patients in our hospital,
in 2005 the department of Nephrology initiated a new PD program for the
treatment of end-stage kidney disease, and the following steps were taken to
build the medical collaboration program with PCPs to grow Peritoneal dialysis.
1. CKD
Prevention Collaboration System: We repeatedly held study sessions with
PCPs, explaining about CKD and the importance of early referrals emphasizing
that the patient will be reverse referred to the PCP along with advice on
examinations and treatment policies as specialists (Figure 1). Thus, 2 to 3
years after the study sessions began, early and timely referrals began to be
received by our hospital.
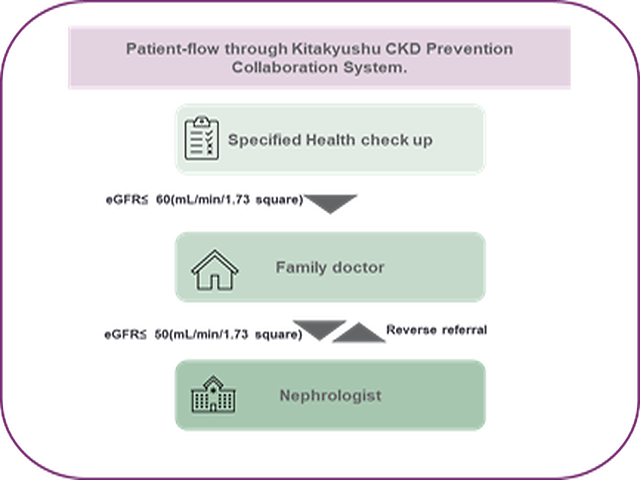
Figure 1: Kitakyushu City CKD
Prevention Collaboration System
2.
Increasing Enrollment of Patients to PD Program
through education and awareness: at our center, all CKD patients are
referred to pre-ESRD education classes regardless of their CKD stage. A teamwork
based educational approach consisting of nephrologists, nurses, dietician,
pharmacist, social worker, physical therapist, psychologist educate and help
patients and families understand various treatment options. This allows planned
initiation of the appropriate RRT modality. We also developed a PD Initiating
Program for patients as early as CKD stage 4 with an eGFR<30, that englobes
education about different RRT modalities and SDM consultations at different
stage until RRT decision, at least 3 SDM consultations by doctors and nurses
are planned before admission to start PD or catheter insertion.
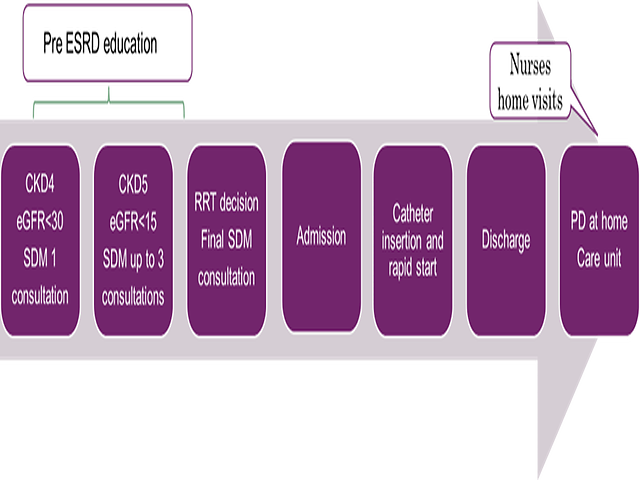
Figure 2: pre-ESRD
patient education and PD Initiating Program at KMH
3. Nephrologists/
PCPs PD collaboration: as the number of patients grew, a PD
collaboration model was created and started as the next step. Unlike HD where
the patient is managed in the dialysis clinic, PD patient can be managed by the
PCP, due to different incentive and reimbursement policies, resulting in referrals
spurred in the early CKD stage to our hospital and growth of PD patients.
This
cooperation system includes PCPs education programs and seminars, study
sessions and conferences, explanations of patient centric care, advantages of
PD from an economic standpoint and PD reimbursement system.
PCP’s role was
clearly defined, consisting of a bimonthly patient visit that includes a weight
check, amount of fluid removed, salt and fluid intake status, infection
prevention with exit site check and blood test prescription and check, with the
reassurance of hospital availability 24h/7day in case of emergency or when the
PD prescription needs adjustment. The patients still need to visit our facility
once every three months for regular checkups, for PET biannually and for transfer
set. In addition, during these visits we also reviewed dialysis prescriptions,
and staff members re-educated patients, their families and their support
persons regarding PD, and examined cardiovascular diseases non-invasively.
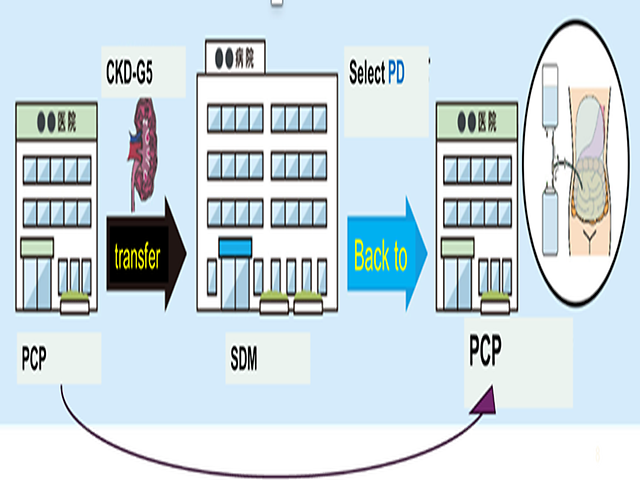
Figure 3: PCPs and Nephrologists
collaboration model in PD
