 Baseline Population Characteristics:
Baseline Population Characteristics:
Both groups were comparable at baseline in terms of demographic and clinical characteristics. The mean age was 57 years, males predominated (59.4%), and type 2 diabetes was the primary etiology of CKD in 81.3% of patients. There were no significant differences in baseline erythropoietin use between the groups.
Primary Outcome:
Significant Increase in Residual Uresis
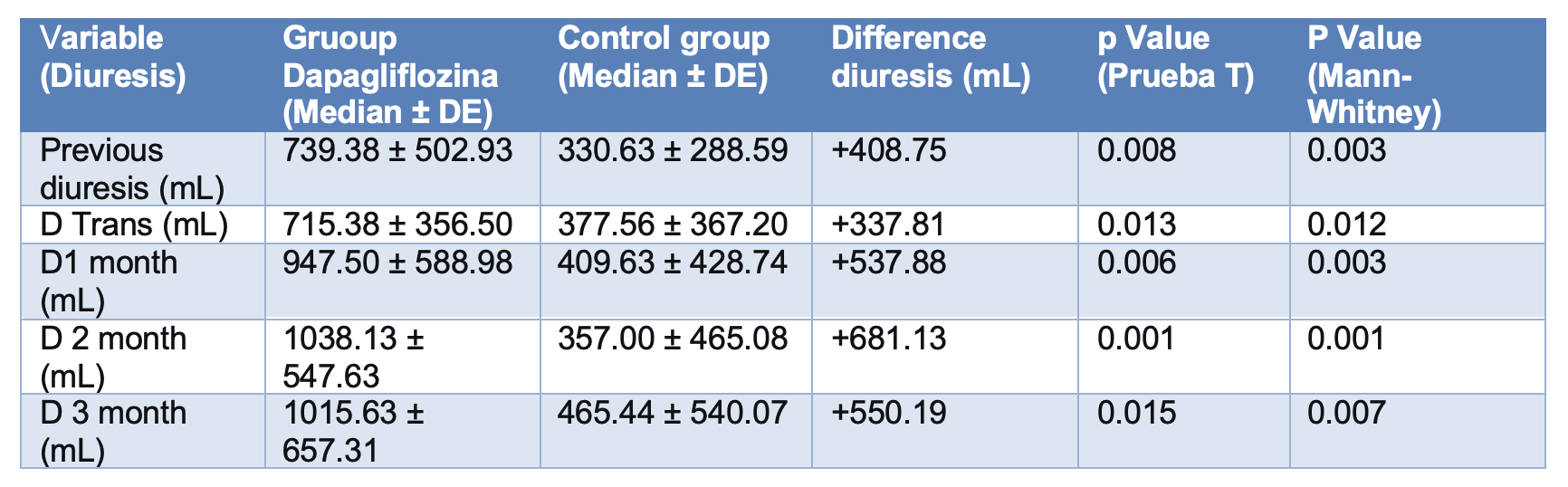
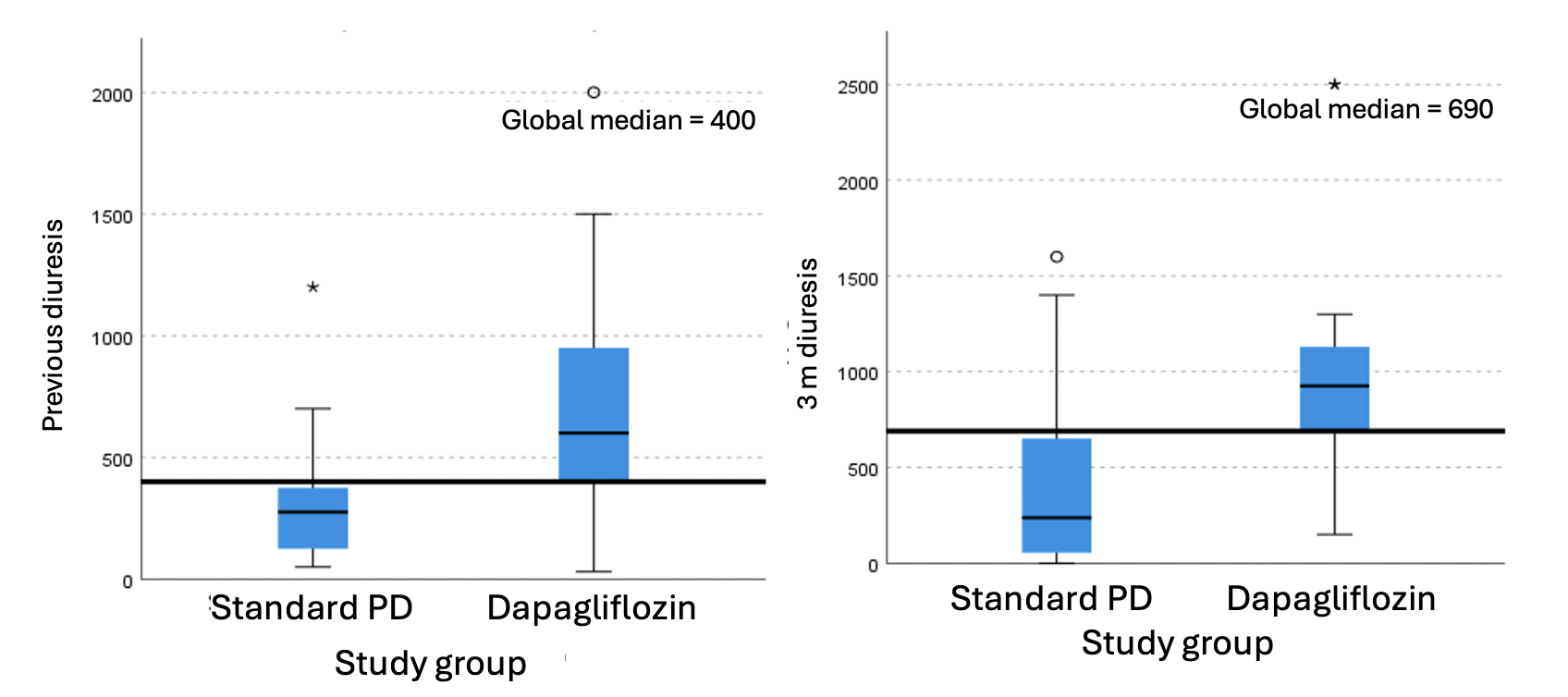
The analysis revealed a statistically significant difference in residual uresis favoring the dapagliflozin group at all measurement points.
• During Hospitalization: The dapagliflozin group had a mean uresis of 715.38 ± 356.5 ml, compared to 377.56 ± 367.20 ml in the control group. This represents a mean difference of +337.81 ml (p=0.003) in favor of the intervention group from the early stages.
• At Month 1: The gap widened. Mean uresis in the case group was 947.50 ± 588.98 ml, while in the control group it was 409.63 ± 428.74 ml, with a mean difference of +537.88 ml (p=0.003).
• At Month 2: The difference peaked. The dapagliflozin group averaged 1038.13 ± 547.63 ml, versus 357.00 ± 465.08 ml in the control group, representing a mean difference of +681.13 ml (p=0.001).
• At Month 3 (End of Follow-up): Superiority was maintained. The intervention group had a uresis of 1015.63 ± 657.31 ml, compared to 465.44 ± 540.07 ml in the control group, with a mean difference of +550.19 ml (p=0.007).
Nonparametric analysis confirmed these findings, reporting a median between-group difference of +585 ml (95% CI: 190–880 ml) in favor of the dapagliflozin group at month 3. These results strongly demonstrate that dapagliflozin not only preserves but significantly increases residual uresis in patients starting peritoneal dialysis.
Secondary Outcomes:
Glomerular Filtration Rate
A modest and statistically significant improvement was observed only in the first month in the dapagliflozin group (+2.45 ml/min/1.73 m², p=0.013). This difference lost statistical significance in the second and third months, suggesting that the main effect was not on stable eGFR, but on urinary flow.
Hemoglobin and Erythropoietin Use: A trend toward increased hemoglobin was identified in the intervention group at month three (12.03 g/dL vs. 10.58 g/dL), with a difference of +1.45 g/dL, although this difference did not reach statistical significance (p=0.096). There were no significant differences in the dose of erythropoietin used.
Safety and Tolerance: The safety profile of dapagliflozin was excellent. Only one case of peritonitis was recorded in the intervention group (6.25% vs. 0% in the control group, p=1.000), with no significant association. No urinary tract or respiratory infections, episodes of severe hypoglycemia, or ketoacidosis were reported. Drug tolerance was 100%, with no discontinuations due to adverse effects.
