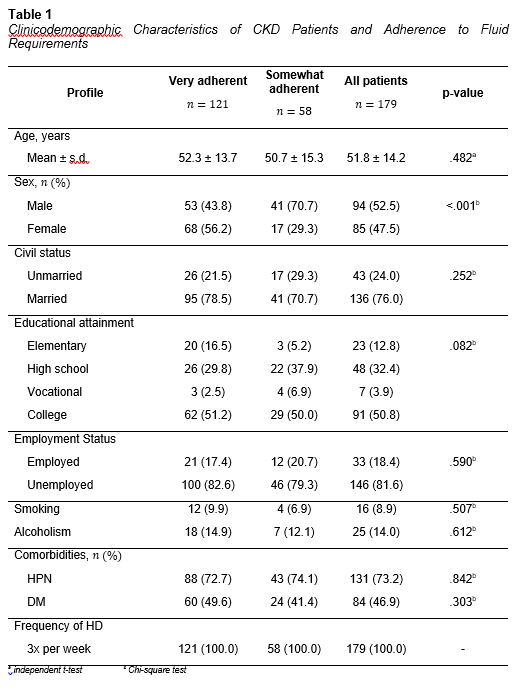
Table 1 presents the clinicodemographic characteristics of chronic
kidney disease (CKD) patients categorized according to their adherence to fluid
restrictions, subdivided into “very adherent” and “somewhat adherent” groups,
with a total sample size of 179 patients. The mean age of the patients was
comparable across the two adherence groups, with those very adherent having a
mean age of 52.3 ± 13.7 years and those somewhat adherent 50.7 ± 15.3 years,
with no statistically significant difference observed (p = 0.482).
Regarding sex distribution, a significant difference was noted
between groups (p < 0.001). The very adherent group had a higher proportion
of females (56.2%) compared to the somewhat adherent group, where males
predominated at 70.7%. Civil status did not significantly differ between adherence
groups (p = 0.252), with the majority being married in both groups (78.5% in
very adherent and 70.7% in somewhat adherent). Educational attainment showed no
statistically significant difference (p = 0.082), though more patients in the
very adherent group attained college education (51.2%) compared to 50.0% in the
somewhat adherent group.
Employment status was largely similar between groups (p = 0.590),
with most patients unemployed (approximately 80% in each group). Lifestyle
factors such as smoking (p = 0.507) and alcoholism (p = 0.612) showed no
significant differences between groups. Comorbidities, including hypertension
and diabetes mellitus, were highly prevalent but did not differ significantly
between adherence groups. Specifically, hypertension was present in 72.7% of
very adherent patients and 74.1% of somewhat adherent patients (p = 0.842),
while diabetes mellitus was found in 49.6% of very adherent versus 41.4% of
somewhat adherent patients (p = 0.303).
All patients in the study underwent hemodialysis thrice weekly.
Overall, the data indicate that sex is the only clinicodemographic
characteristic significantly associated with adherence to fluid restrictions
among CKD patients, with females more likely to be very adherent. Other factors
such as age, civil status, educational attainment, employment status, lifestyle
habits, and comorbidities showed no significant association with fluid
adherence in this cohort.
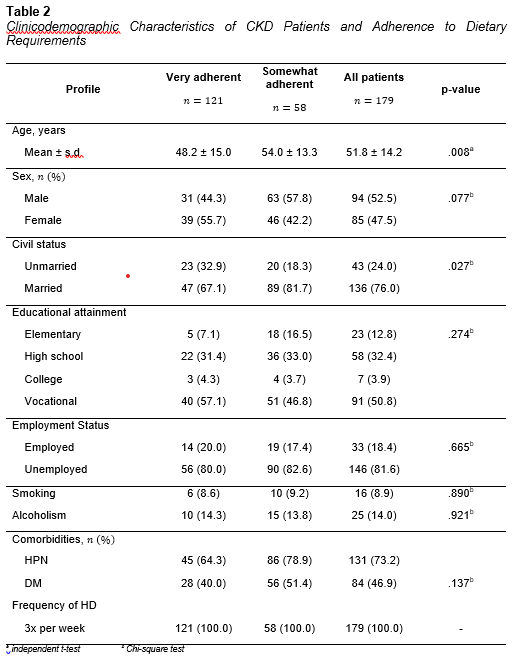
The
clinicodemographic characteristics of chronic kidney disease patients were
analyzed according to their adherence to dietary requirements, dividing them
into very adherent and somewhat adherent groups. The mean age differed
significantly between the groups, with the very adherent patients being younger
(48.2 ± 15.0 years) compared to the somewhat adherent group (54.0 ± 13.3
years), yielding a p-value of 0.008.
Sex distribution showed no statistically significant difference (p
= 0.077), although a higher proportion of females was observed in the very
adherent group (55.7%) compared to 42.2% in the somewhat adherent group. Civil
status revealed a statistically significant association with dietary adherence
(p = 0.027), where a larger percentage of married patients were somewhat
adherent (81.7%) versus very adherent (67.1%), while the unmarried proportion
was higher among the very adherent.
Educational attainment did not significantly differ between groups
(p = 0.274). Vocational education was the most common level attained by both
adherence groups, followed by high school and elementary education. Employment
status was similar across groups (p = 0.665), with the majority unemployed in
both groups.
Lifestyle factors such as smoking (p = 0.890) and alcoholism (p =
0.921) did not significantly influence dietary adherence. The prevalence of
comorbidities such as hypertension and diabetes mellitus was also comparable
between groups, with no statistically significant differences (p = 0.137 for
DM). All patients underwent hemodialysis three times weekly.
Overall, younger age and civil status show significant
associations with dietary adherence, with younger and unmarried patients more
likely to be very adherent to dietary restrictions. Other clinicodemographic
factors including sex, education, employment, lifestyle habits, and
comorbidities did not demonstrate significant differences between dietary
adherence groups.
The
analysis of common barriers to adherence to dietary and fluid restrictions
among chronic kidney disease patients identified three primary factors.
Cravings were the most frequently reported barrier, affecting 44% of patients,
indicating a strong desire or urge to consume restricted foods or fluids
despite clinical recommendations. Weather factors were the second most common
barrier, affecting 38% of patients, reflecting environmental conditions that
may influence patients’ ability or willingness to adhere to restrictions.
Financial constraints were reported by 18% of patients, highlighting economic
limitations as a less common but still significant factor hindering compliance
with prescribed dietary and fluid restrictions. These findings underscore the multifaceted
challenges patients face in managing dietary and fluid adherence, suggesting
the need for comprehensive support addressing behavioral, environmental, and
socioeconomic dimensions.

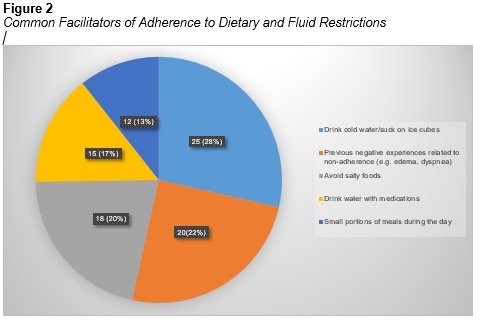
The
facilitators of adherence identified in this study highlight several practical
and psychological strategies employed by hemodialysis patients. Drinking cold
water and sucking on ice cubes (reported by 28%) serve as effective means to
manage thirst, a common challenge in fluid restriction, by providing oral
cooling and reducing the sensation of dryness. Fear of experiencing previous
unpleasant symptoms such as fluid overload or discomfort (22%) acts as a strong
psychological motivator, reinforcing adherence through recognition of negative
health consequences. Behavioral strategies like avoiding salty foods (20%),
drinking water alongside medications (17%), and consuming small portions of
meals throughout the day (13%) illustrate patients’ conscious efforts to
control fluid and dietary intake in manageable ways.
Overall, these facilitators suggest that patients leverage both
behavioral adaptations and psychological motivations to support adherence,
aligning with literature emphasizing motivation, self-efficacy, and practical
coping strategies as key drivers of treatment compliance. Encouraging such
patient-initiated strategies in clinical practice can enhance adherence,
improve symptom control, and ultimately contribute to better clinical outcomes in
the hemodialysis population.
The
study’s findings offer a comprehensive understanding of the multifaceted
factors influencing adherence to fluid and dietary restrictions among chronic
kidney disease (CKD) patients undergoing hemodialysis (HD). These insights not
only highlight demographic associations but also illuminate both barriers and
facilitators that shape patients’ adherence behaviors, underscoring the
complexity of managing this vulnerable population.
Demographic Influences on Adherence
Sex
differences emerged as a significant predictor of fluid adherence, with female
patients more likely to comply with fluid restrictions than males. This finding
corroborates prior evidence indicating gender disparities in health behaviors, where
women often engage more actively in self-care practices (Karamanidou et al.,
2018; Schmidt et al., 2016)10,11. Biological, psychological, and
sociocultural factors may underlie this pattern, including greater health
consciousness and adherence motivation in females. Conversely, males may
benefit from targeted interventions addressing their unique psychosocial
contexts and potential risk-taking tendencies to close this adherence gap.
Regarding
dietary adherence, younger age and unmarried status were associated with better
compliance. Older patients frequently face cognitive, functional, and social
challenges that complicate adherence to complex dietary regimens (Szabo et al.,
2017)12. The influence of marital status may reflect family
dynamics—for married patients, shared meals and social eating behaviors can
challenge dietary restrictions, while unmarried patients may experience more
autonomy in food choices (Slomka & Metlay, 2010)13. These
demographic findings stress the need for culturally sensitive, age-appropriate
educational approaches and family-inclusive counseling to foster dietary
adherence.
Barriers to Adherence
The
study’s identification of cravings, weather-related factors, and financial
constraints as top barriers aligns well with existing literature. Cravings are
a universally reported challenge in restrictive diets, often driven by
physiological hunger signals and psychological stress (Knafl & Grey, 2015)14.
Behavioral interventions such as cognitive-behavioral therapy or motivational
interviewing can help patients develop coping skills to resist cravings (Crist
& Weiner, 2017)15.
Weather-related
factors as barriers are less commonly documented but intuitively important.
Extreme heat may exacerbate thirst, aggravating fluid management difficulties,
while adverse weather can impact accessibility to care or food supplies (Keller
et al., 2012)16. Recognizing such environmental influences calls for
adaptive patient education and support, including guidance on managing thirst
during hot weather, and ensuring continuity of care despite environmental
challenges.
Financial
limitations, although reported less frequently, remain a critical factor.
Economic hardship restricts access to recommended foods and dialysis-related
supplies, contributing to nonadherence and poorer outcomes (Flythe et al.,
2019)17. Addressing this through social support services, subsidy
programs, or community resources is essential in comprehensive care.
Facilitators of Adherence
The
novel addition of facilitators in this study deepens the understanding of
patient-centered strategies that promote adherence. The use of cold water and
ice cubes by 28% of patients is a practical behavior supported by clinical
guidance to alleviate thirst while limiting fluid intake (Mailani et al., 2021)18.
This simple intervention can be emphasized in patient education as a
manageable, non-pharmacological technique.
Fear
of previous unpleasant symptoms motivated 22% of patients, highlighting the
importance of experiential learning and symptom recognition in adherence.
Patients who associate adherence with avoidance of distressing symptoms such as
fluid overload or dyspnea may demonstrate higher compliance due to increased
perceived severity and susceptibility (Welch, 2001)19. Clinicians
should leverage this by reinforcing the causal link between adherence and
symptom prevention during counseling.
Avoidance
of salty foods (20%), drinking water with medications (17%), and eating small,
frequent meals (13%) reflect intentional behaviors to adhere within daily life
constraints. These strategies align with established recommendations to control
sodium intake, manage fluid load concomitant with medication schedules, and
moderate nutrient intake to avoid metabolic imbalances (Clark-Cutaia et al.,
2014; Sulistyaningsih et al., 2020)20,21. Encouraging such adaptive
behaviors can help patients feel empowered and supported in adherence.
