 The patient was a 43-year-old Filipino male with biopsy-proven biliary tuberculosis diagnosed earlier in 2024. He initially presented with progressive jaundice, generalized weakness, and later, a new-onset seizure. Over the preceding months, he had been treated with several anti-TB regimens, each modified in response to rising liver enzyme levels and worsening jaundice. Despite drug substitutions, his condition deteriorated, prompting transfer to East Avenue Medical Center for further evaluation and management.
The patient was a 43-year-old Filipino male with biopsy-proven biliary tuberculosis diagnosed earlier in 2024. He initially presented with progressive jaundice, generalized weakness, and later, a new-onset seizure. Over the preceding months, he had been treated with several anti-TB regimens, each modified in response to rising liver enzyme levels and worsening jaundice. Despite drug substitutions, his condition deteriorated, prompting transfer to East Avenue Medical Center for further evaluation and management.
His past medical history revealed that in March 2024, fatty liver changes were detected on imaging. By May, he reported pruritus and unintentional weight loss, but no medical consultation was sought. When symptoms persisted, he sought treatment in Auckland, New Zealand, where imaging revealed intrahepatic biliary abnormalities, right hepatic lobe atrophy, and chronic portal vein thrombosis. ERCP confirmed biliary tuberculosis, and a liver-sparing regimen was initiated. However, hepatic deterioration continued even after adjustments to minimize drug toxicity. Upon returning to the Philippines, he resumed anti-TB therapy, which included hepatotoxic agents, leading to further biochemical derangement.
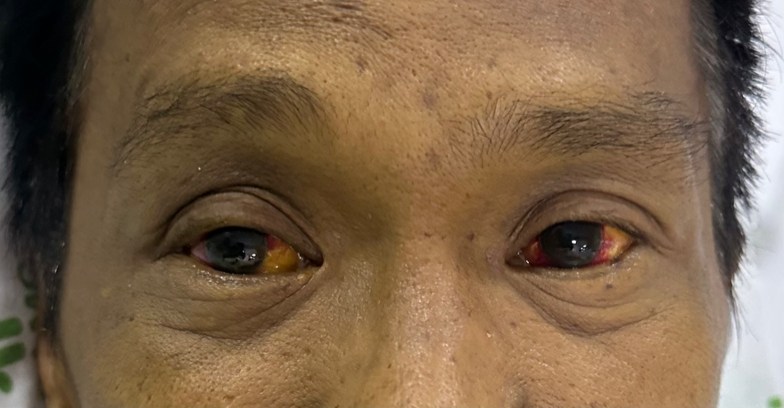
On presentation, he was conscious and oriented, with stable vital signs but marked jaundice, ascites, and multiple bruises suggestive of bleeding diathesis. His laboratory findings were consistent with acute liver failure: prothrombin time (PT) activity less than 5%, INR greater than 6, activated partial thromboplastin time (APTT) over 200 seconds, and markedly elevated bilirubin levels (total bilirubin 567 µmol/L, direct 415 µmol/L, indirect 151 µmol/L). Transaminases were elevated (AST 285 U/L, ALT 164 U/L), and anemia was present (hemoglobin 84 g/L), with leukocytosis and reactive thrombocytosis. Electrolyte results showed mild hyponatremia (129 mmol/L) and low magnesium (0.83 mmol/L), while renal function was preserved. Imaging from prior hospitalization confirmed intrahepatic biliary strictures, right lobe atrophy, and chronic portal vein thrombosis. Serologic testing for hepatitis B was negative.
The diagnosis of fulminant hepatic failure was made, likely secondary to cumulative hepatotoxicity from anti-TB drugs on a background of biliary tuberculosis and vascular compromise. Management focused on stabilizing liver function and providing supportive care. Fresh frozen plasma and packed red blood cell transfusions were given to address coagulopathy and anemia. Because transplantation was not feasible, DPMAS therapy was initiated as a bridging intervention.
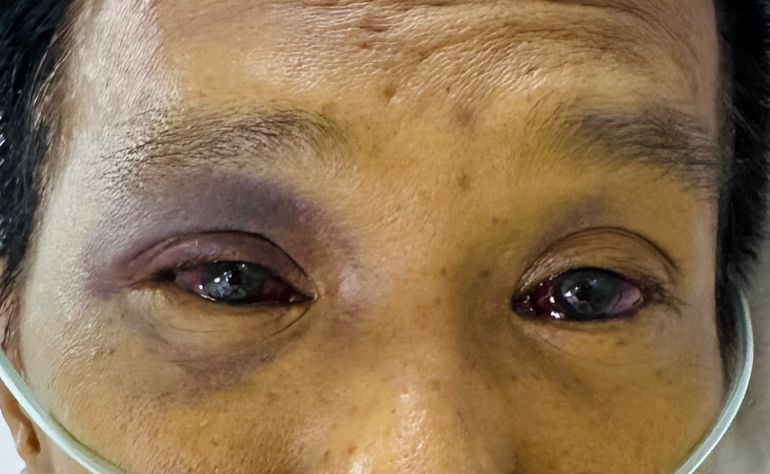
The patient underwent four sessions of DPMAS on January 9, 11, 13, and 18. Each treatment session aimed to reduce serum bilirubin and circulating hepatotoxins. Following therapy, his biochemical and clinical condition improved significantly. Post-DPMAS laboratory results showed normalization of coagulation parameters (PT 11.30 seconds, INR 0.90) and a marked decline in bilirubin levels (total 308 µmol/L, direct 228 µmol/L, indirect 79 µmol/L). The patient’s mental status stabilized, and his jaundice and bleeding manifestations gradually regressed.
During hospitalization, his anti-TB regimen was carefully adjusted to maintain efficacy while minimizing hepatotoxic risk. Moxifloxacin and ethambutol were retained, while other agents were tapered or reintroduced cautiously as liver function improved. No adverse reactions to DPMAS were observed throughout the treatment course. The patient was eventually discharged in stable condition, with ongoing outpatient follow-up showing continued improvement in hepatic function.
