A 55-year-old woman with past medical history for type 2 diabetes
mellitus on insulin, hypertension, current smoker, prior multiple non-diagnostic
imaging-guided needle aspiration biopsies of a periaortic lymph node, past right
robot-assisted laparoscopic nephroureterectomy for urothelial carcinoma in late
2020 for a large renal mass, previous cholecystectomy, partial left mastectomy
for breast cancer, underwent open retroperitoneal lymph node biopsy. There remained
concerns for metastatic urothelial carcinoma. Outpatient medications included
Dapagliflozin 10 mg daily, insulin, glipizide 20 mg daily, Losartan 25 mg
daily, Prazosin 1 mg at bedtime and Dulaglutide 0.75 mg subcutaneous, weekly.
During the open periaortic lymph node biopsy, the left renal vein was
ligated to mobilize the inferior vena cava. The aortocaval
lymphadenopathy immediately inferior to the left renal vein corresponding to
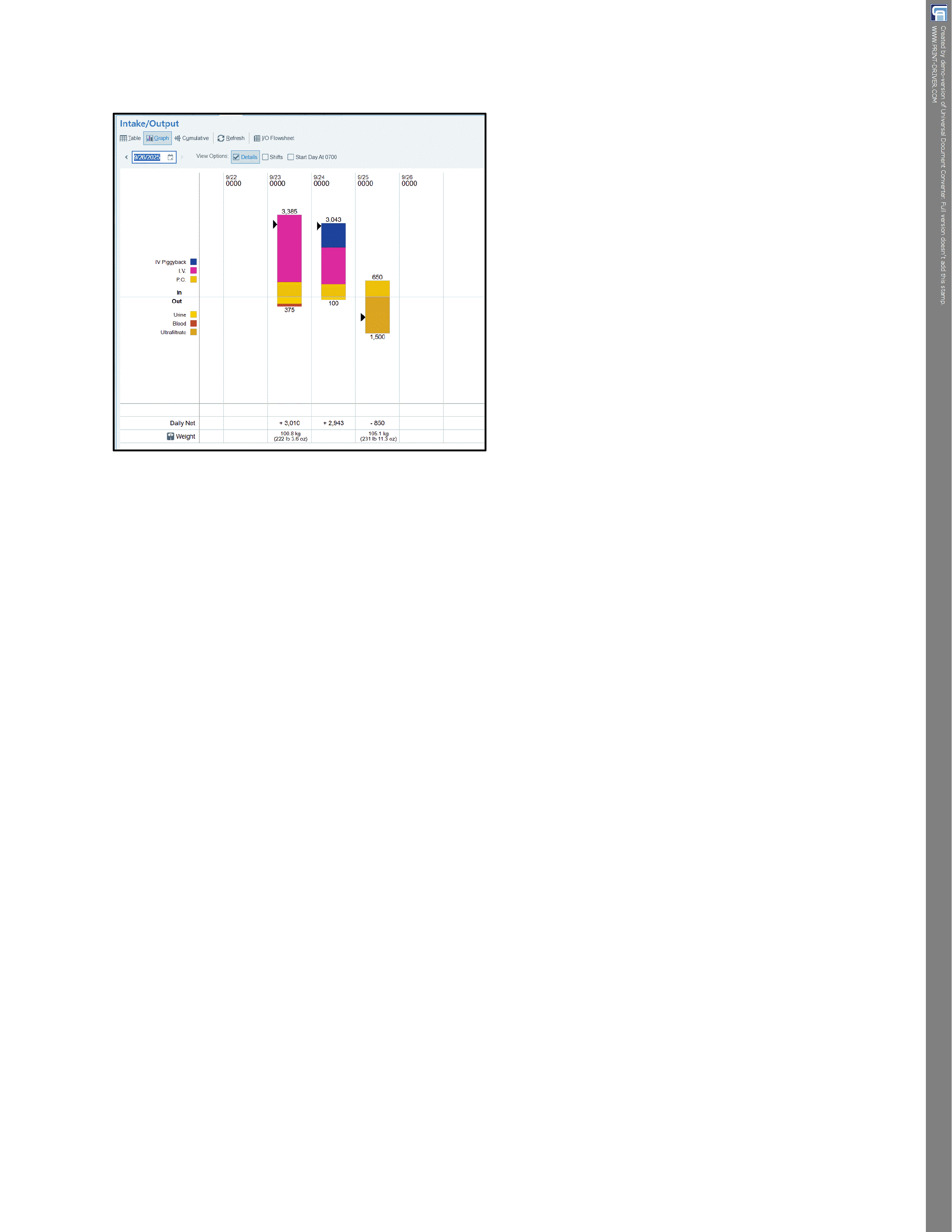
preoperative imaging was removed. Estimated blood loss was 100 mL and
urine output during the surgery was 125 mL. No complications were reported
during the procedure, and the patient tolerated the procedure well and
post-operatively was in hemodynamically stable condition, with a Foley catheter
until ambulatory, and she quickly transitioned to clear liquid diet. The
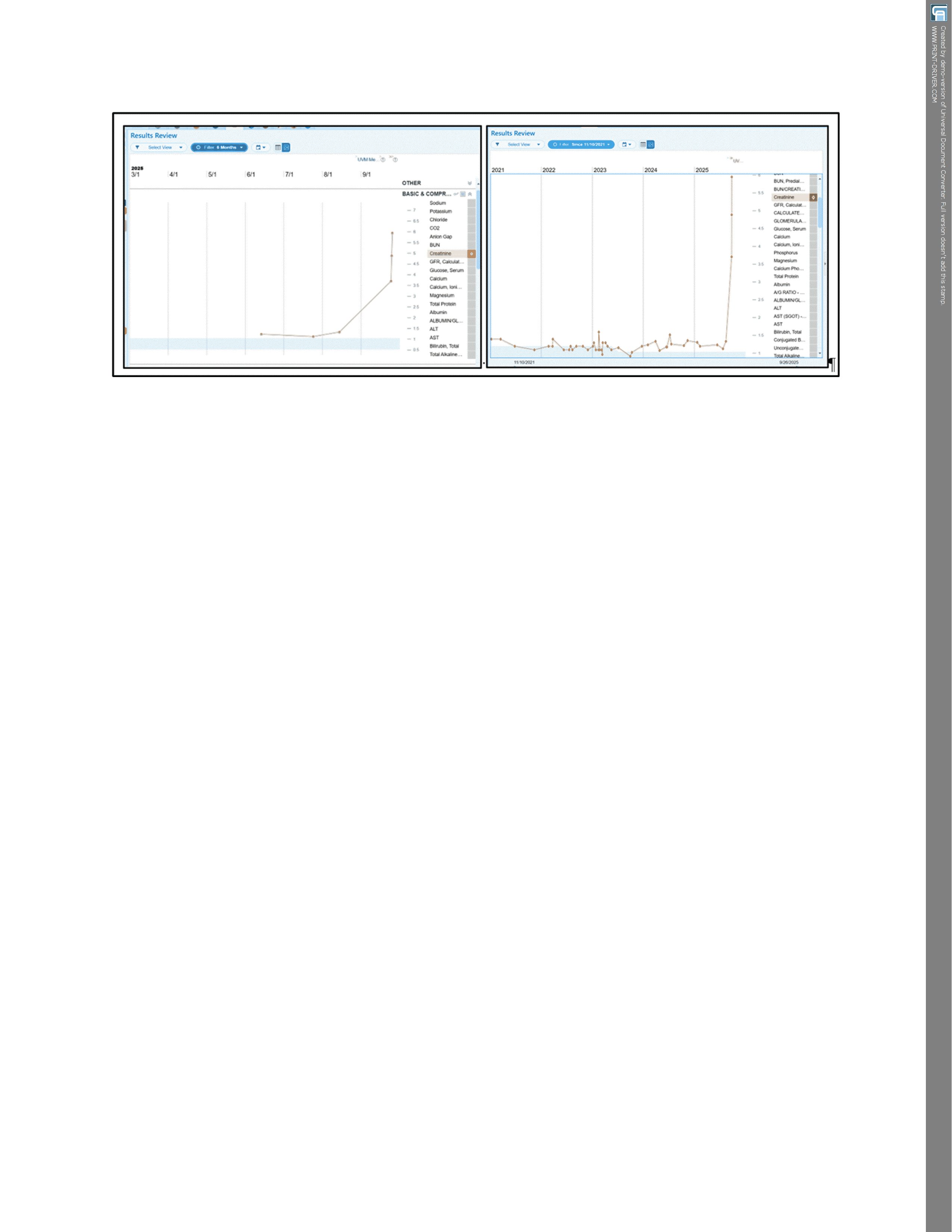
preoperative creatinine was 1.3 mg/dL. Despite stable vital signs, by postoperative
day 1, serum creatinine had almost tripled and quickly rose to 3.71 mg/dL
(FIGURE 1). Creatinine subsequently continued to increase, accompanied by
anuria (FIGURES 1 & 2). Nephrology was quickly consulted on post-operative
day 1. At this point, she was suspected of having irreversible loss of renal
function. A urine bladder scan that morning on post-operative day 1 revealed
zero urine and the Foley catheter was empty. Except for post-operative abdominal pain, she had no
systemic symptoms, no fever or chills, no nausea or vomiting but no urine
output. Physical examination was normal except for post-op abdominal status.
She had no peripheral edema. A tunneled hemodialysis catheter was promptly placed on postoperative day
1 and she had her first hemodialysis treatment on postoperative day 2.
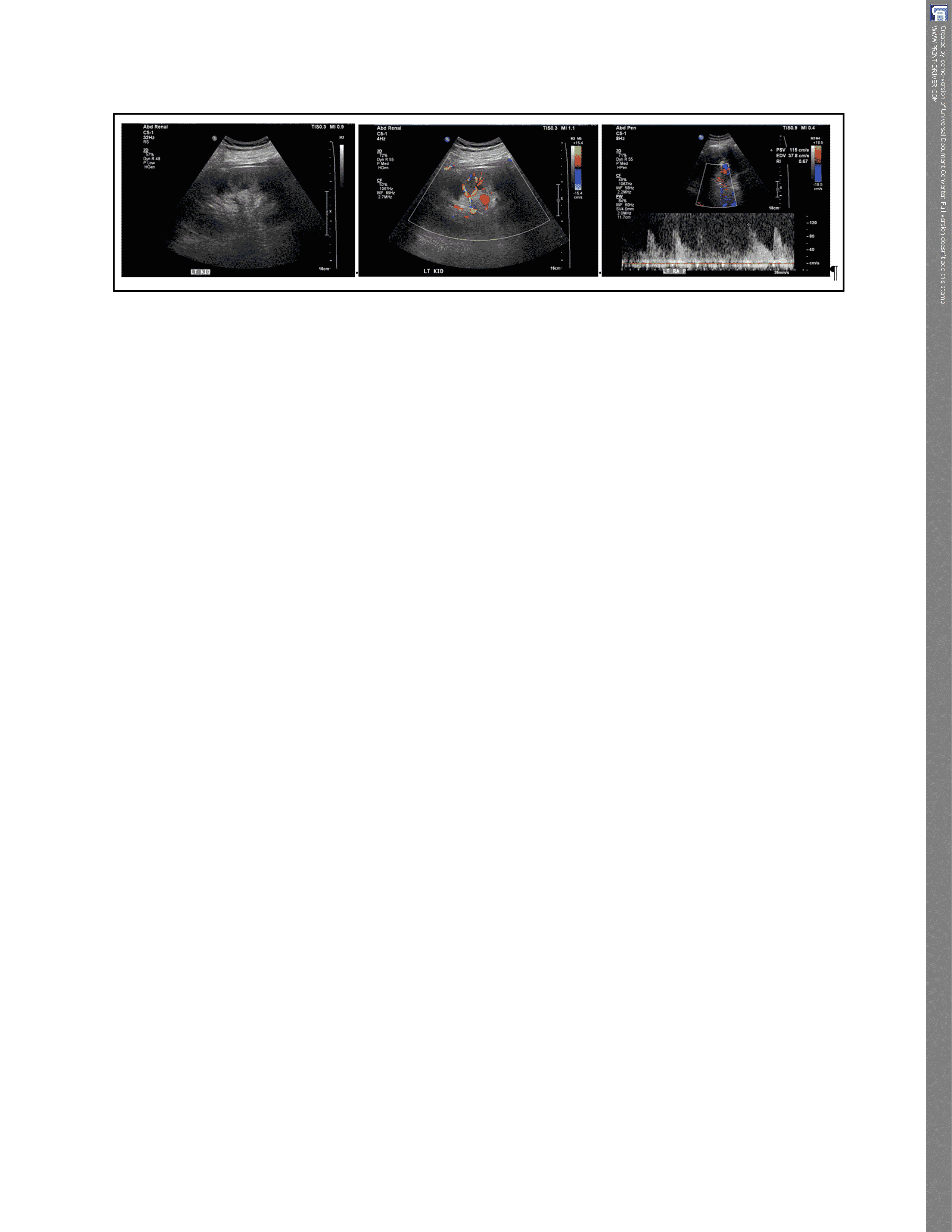
At
the same time, a renal ultrasound examination with renal artery and vein Duplex
was completed on post-operative day 1 to assess the renal vascular anatomy and
physiology. Left kidney size before nephrectomy in early 2022 by ultrasound
measured 13.4 cm in length. This time around, the left kidney measured 15 cm
and Duplex exam showed no evidence for renal artery stenosis (FIGURE 3).
Proximal left renal peak systolic velocity in early 2022 was 275 cm/s whereas
proximal left renal artery peak systolic velocity this time around was reduced
to 115 cm/s. The left renal vein was visualized distally and was widely patent
(FIGURE 3).
With
renewed production of urine on post-operative day 3, urinalysis by dipstick
revealed clear yellow urine with SG 1.014, pH 5.5, 2+ blood, 3+ proteinuria,
negative glucose, 4-9 WBC/HPF, 3-10 RBC, no bacteria and <10 casts/HPF.
There were a few renal epithelial cells on urine deposit microscopy.
She
received alternate daily hemodialysis treatments for persistent oligo-anuria.
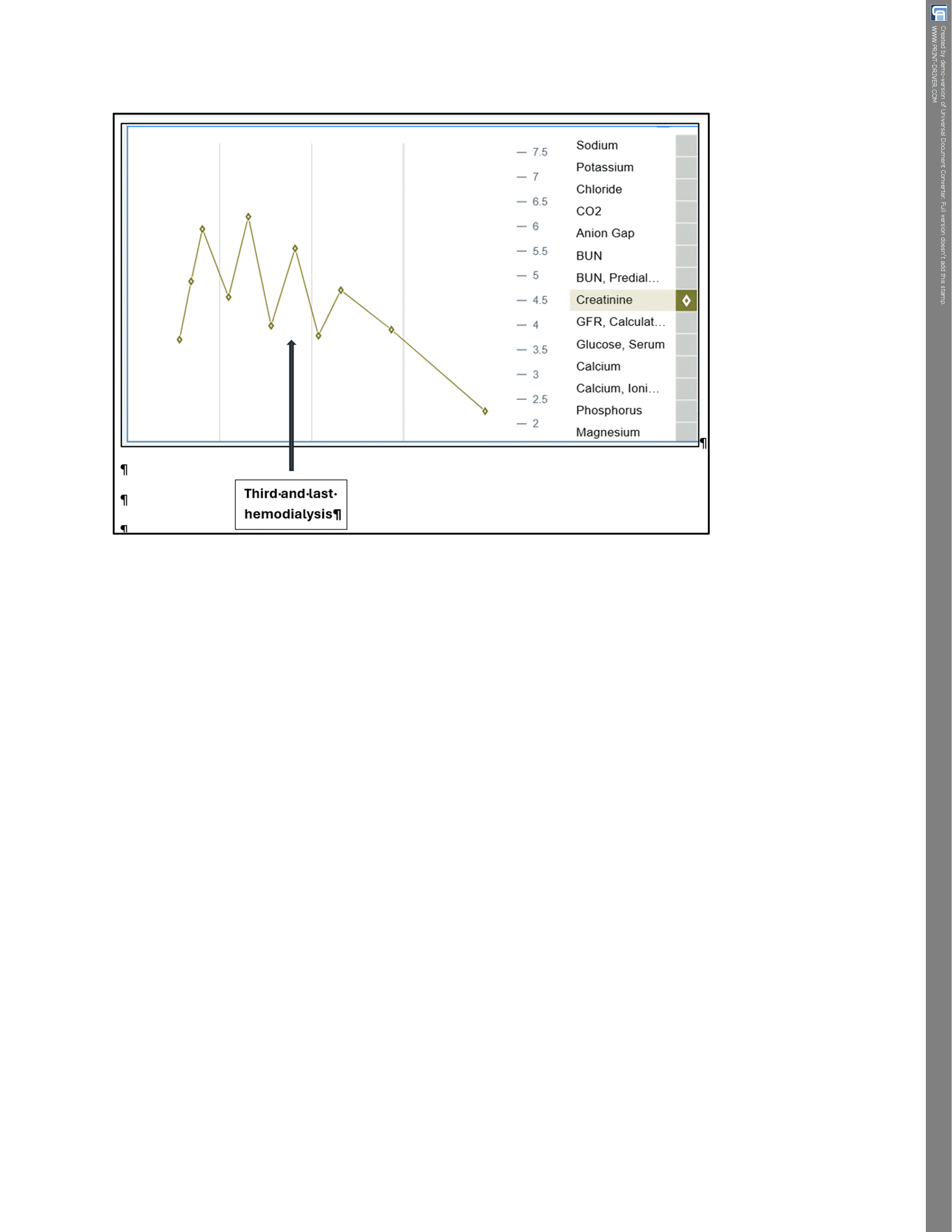
Serum creatinine peaked at 6.2 mg/dL o post-operative day 4 (FIGURE 4). In
total, she received 3 hemodialysis treatments. Serum
creatinine and BUN were simply returning back upwards between the alternate
daily 3-hr hemodialysis treatments. (FIGURE 4). The third and the last hemodialysis
treatment was on post-operative day 6. By the next day, she was making a lot
more urine and she was therefore discharged home after 8 days in the hospital, on
postoperative day 7, with close monitoring. She never needed additional renal
replacement therapy. Indeed, serum creatinine had started to decrease
spontaneously, without the need for more hemodialysis (FIGURE 4).
Hyperphosphatemia has since normalized.