A total of 51 critically ill patients with pregnancy-related
acute kidney injury (PRAKI) and anaemia were evaluated. The mean age was 27.7 ±
5.3 years. None of the patients had pre-existing comorbidities except two—one
with chronic heart failure and the other with chronic kidney disease. Regarding
antenatal care, 31 patients (60.78%) were booked, while 20 (39.21%) were
unbooked. In terms of obstetric profile, 17 patients (33.33%) were primigravida
and 34 (66.67%) were multigravida. Among these patients, 31(60.07%) underwent
emergency lower segment caesarean section (LSCS), 2 (3.90%) had elective LSCS, and
16 (31.37%) delivered vaginally. A total of 41 patients (80.39%) delivered
preterm, i.e., before 37 weeks of gestation.
There were 35 (68.60%) survivors and 16 (31.30%)
non-survivors. The median SOFA score at admission was 10, and the median
APACHE-2 score was 21. All patients except 3 required mechanical ventilator
support during their ICU stay. The median duration of mechanical ventilation
was 4 days. Thirty-six patients (76.50%) required vasopressor support either at
admission or during their hospital stay. {Table 1}
Table 1:Basic
Demographic profile
|
Variable
|
Number of patients (%)
|
|
Mean Age (years)
|
27.7 ± 5.3 years
|
|
Pre-existing Comorbidities
|
2 patients (1 CHF, 1 CKD)
|
|
Booked Cases (Antenatal Care)
|
31 (60.78%)
|
|
Unbooked Cases
|
20 (39.21%)
|
|
Primigravida
|
17 (33.33%)
|
|
Multigravida
|
34 (66.67%)
|
|
Emergency LSCS
|
31 (60.07%)
|
|
Elective LSCS
|
2 (3.90%)
|
|
Vaginal Delivery
|
16 (31.37%)
|
|
Preterm Deliveries (<37 weeks)
|
41 (80.39%)
|
|
Survivors
|
35 (68.60%)
|
|
Non-survivors
|
16 (31.30%)
|
|
Median SOFA Score at Admission
|
10
|
|
Median APACHE II Score
|
21
|
|
Mechanical Ventilation Required
|
48 (94.1%)
|
|
Median Duration of Mechanical Ventilation (days)
|
4
|
|
Vasopressor Support Required
|
36 (76.50%)
|
|
Mean Serum Creatinine at Admission (mg/dL)
|
3.3
|
|
Dialysis Support Required
|
23 (45.09%)
|
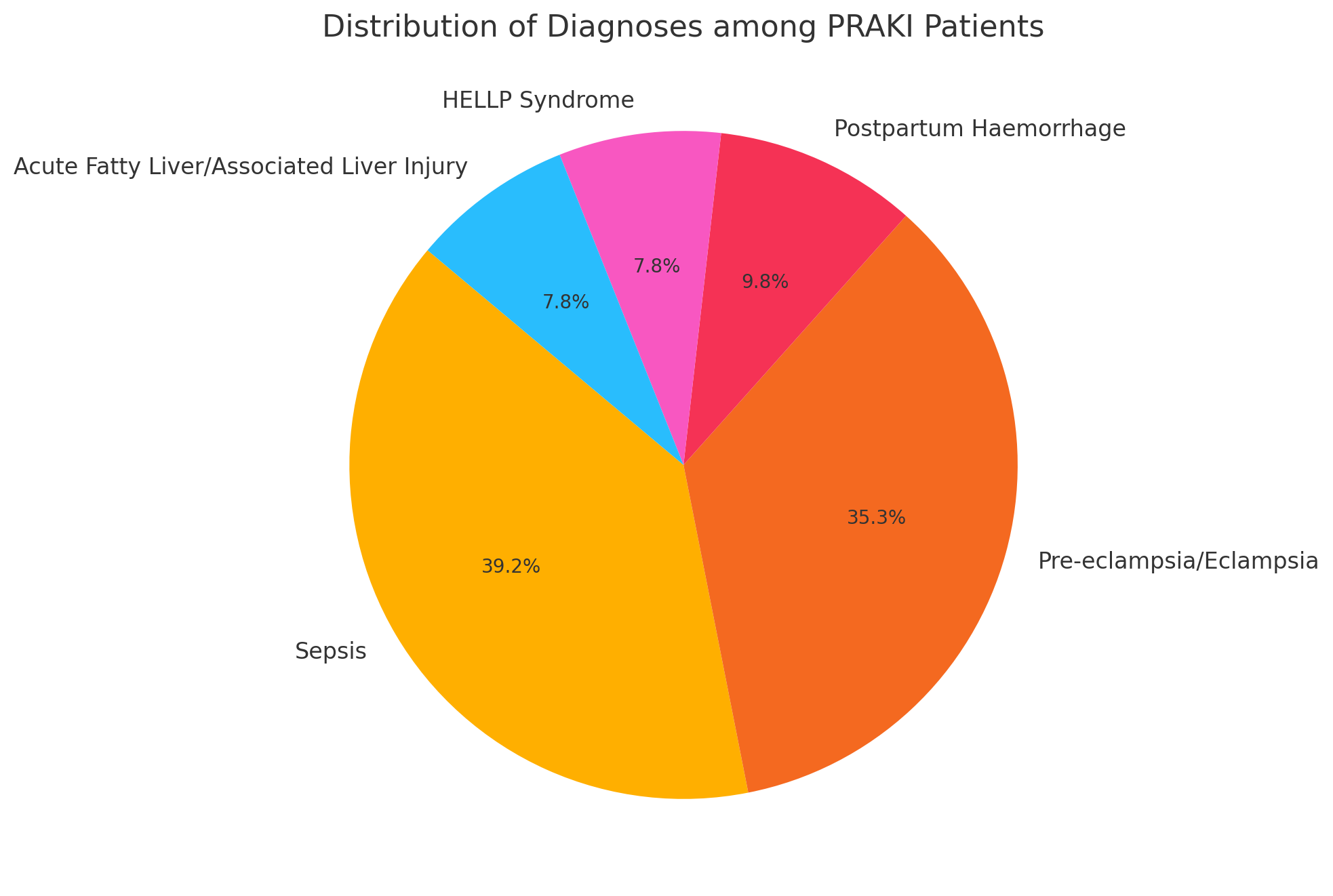
The most common diagnoses were sepsis (39.21%),
pre-eclampsia/eclampsia (35.29%), postpartum haemorrhage (9.80%), HELLP
syndrome (7.84%), and acute fatty liver/associated liver injury (7.84%),
emphasising sepsis and hypertensive disorders as leading causes of PRAKI. The
mean serum creatinine at admission was 3.3 mg/dL, confirming moderate-to-severe
renal dysfunction. Among all patients, 23 (45.09%) required dialysis support.
{Figure 1}
Figure 1: Distribution of Diagnosis among PRAKI patients
The mean haemoglobin level at admission was 7.70 ± 2.09
g/dL, with a mean MCV of 85.33 ± 9.61 fL. At discharge (or death), the mean haemoglobin
was 8.09 ± 6.50 g/dL, and the mean MCV was 84.15 ± 14.8 fL, indicating
persistent moderate-to-severe anaemia. Peripheral smear evaluation at admission
revealed normocytic normochromic anaemia in 32 patients (62.70%), microcytic
hypochromic anaemia in 12 patients (23.50%), and a mixed anaemia pattern in 7
patients (13.70%). Features of microangiopathic haemolytic anaemia (MAHA) were
observed in 8 patients. {Table 2,3}
Table 2 :Hematological
parameters of PRAKI patients
|
Red Cell Morphology
|
Mean +/- SD
|
|
Mean Haemoglobin at Admission (g/dL)
|
7.70 ± 2.09
|
|
Mean MCV at Admission (fL)
|
85.33 ± 9.61
|
|
Mean Haemoglobin at Discharge/Death (g/dL)
|
8.09 ± 6.50
|
|
Mean MCV at Discharge/Death (fL)
|
84.15 ± 14.8
|
Table 3:
General Blood picture of patients
|
General Blood Picture
|
Number of Patients (%)
|
|
Peripheral Smear - Normocytic Normochromic
|
32 (62.70%)
|
|
Peripheral Smear - Microcytic Hypochromic
|
12 (23.50%)
|
|
Peripheral Smear - Mixed Anaemia
|
7 (13.70%)
|
|
Features of MAHA Observed
|
8 (15.68%)
|
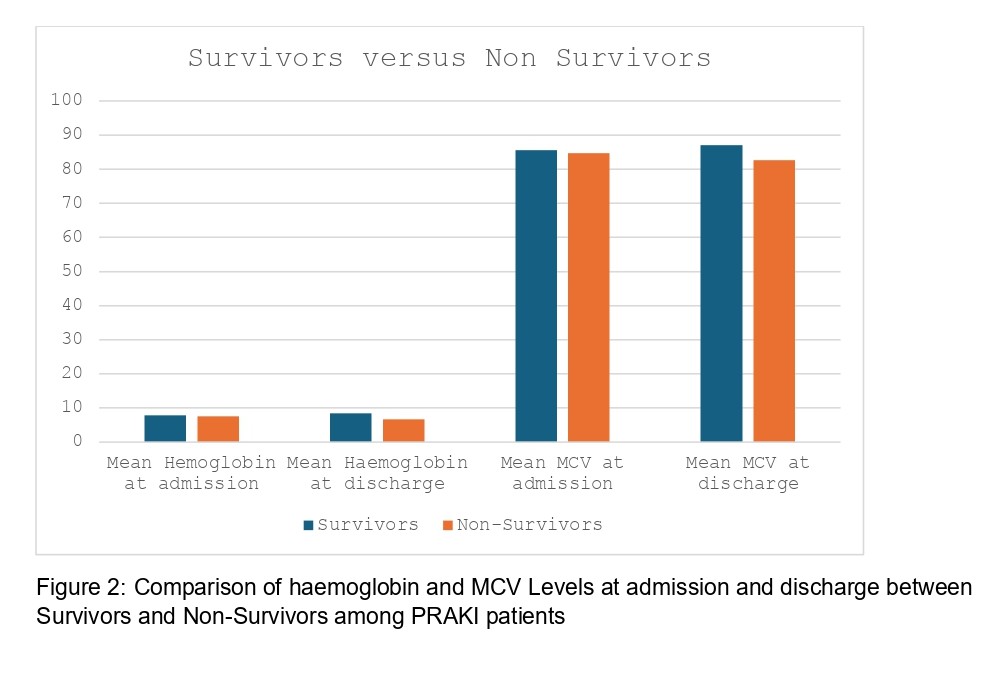
The mean haemoglobin at admission among survivors was 7.80
g/dL, compared to 7.54 g/dL among non-survivors. At discharge or death,
survivors had Hb of 8.49 g/dL, while non-survivors had 6.7 g/dL. {Figure 2}. We
compared mean haemoglobin (Hb) and mean corpuscular volume (MCV) between
survivors and non-survivors using an independent two-sample t-test; while
neither Hb nor MCV at admission differed significantly between groups
(p>0.05), survivors had significantly higher Hb at discharge (8.50 ± 1.93 g/dL vs. 7.19 ± 1.36 g/dL, p≈0.008),
whereas MCV differences at discharge were not statistically significant (p≈0.132).
Although differences were modest, lower haemoglobin levels
were associated with a poorer prognosis.
