A 56-year-old male (BMI 20.7 kg/m²) was admitted in August 2024. His medical history began two years prior with increased nocturia. Laboratory tests at that time revealed significantly elevated serum creatinine (415.5 μmol/L) and parathyroid hormone (PTH) levels (2469 pg/ml). 16 months ago, his serum creatinine rose to 908 μmol/L, and he began to receive maintenance hemodialysis. 1 year ago, he developed recurrent massive melena without obvious inducement. After each episode of melena, his hemoglobin level dropped sharply from above 90 g/L to approximately 40 g/L. Gastroscopy identified hiatal hernia, chronic non-atrophic gastritis, and duodenal bulbitis, with no definitive bleeding lesion. Each episode was managed conservatively with fasting, acid suppression, and blood transfusion, leading to the cessation of bleeding and stabilization of hemoglobin. However, these massive melena episodes recurred every 1-3 months, totaling 5 episodes within one year. One week ago, he came to the outpatient clinic with severe right hand pain and cyanosis. His comorbidities included hypertension for over one year, which was well-controlled with regular medication. He had no history of warfarin use or diabetes. Physical examination revealed cyanosis of the right palm and multiple fingertips, with decreased local skin temperature. Key laboratory findings on admission included: hemoglobin 98 g/L, creatinine 390.6 μmol/L (post-dialysis), calcium 2.81 mmol/L, phosphorus 1.83 mmol/L, and PTH 2469 pg/ml. ANA and ANCA were negative. CTA of the right upper extremity (Figure 1) revealed extensive vascular calcification and stenosis involving multiple arteries, including the axillary, ulnar, radial, palmar arches, digital arteries, and the aorta and its major branches, with findings ranging from mild to severe stenosis.
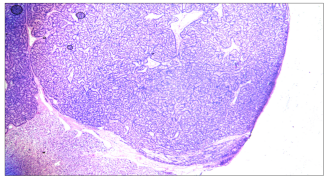
Based on the typical skin lesions, characteristic imaging findings, and existence of risk factors, he was diagnosed with calciphylaxis. Given the recurrent massive gastrointestinal bleeding, an underlying vascular etiology was suspected. A comprehensive treatment regimen was initiated, including sodium thiosulfate, medications to correct calcium-phosphorus metabolism disorders, and parathyroidectomy, in addition to his ongoing maintenance dialysis. Pathological examination of the resected parathyroid tissue confirmed parathyroid hyperplasia (Figure 2). After treatment, the pain and cyanosis in his right hand gradually resolved, and extremity skin temperature returned to normal. During the 15-month follow-up, repeated examinations showed that the PTH levels were suppressed, ranging from 52.75 to 340.7 pg/ml, with serum calcium and phosphorus levels within the normal range. Concurrent with the resolution of the cutaneous ischemic syndrome, his melena ceased and hemoglobin levels gradually increased to 110-125g/L with the same dose of erythropoietin before. This clinical course strongly suggests that the gastrointestinal bleeding was a systemic manifestation of calciphylaxis-induced vasculopathy.
We subsequently conducted a literature review. Using calciphylaxis and gastrointestinal as keywords, we searched the PubMed, Embase, and China National Knowledge Infrastructure (CNKI) databases for case reports of calciphylaxis with gastrointestinal involvement published up to May 2025. The search yielded 12 relevant articles. A comparative analysis of clinical characteristics was performed between these reported cases and the current case.
Combining our case with those from the literature, we summarized 13 cases of calciphylaxis complicated by gastrointestinal bleeding. The patients’ ages ranged from 36 to 76 years, with a median age of 57 years. There were nine females (69.2%) and four males (30.8%). Ten patients (76.9%) had diabetes mellitus, and one was on warfarin. Nine patients underwent hemodialysis, two cases received peritoneal dialysis, and renal replacement therapy was unspecified in two cases. The duration of dialysis ranged from one month to ten years, with the majority exceeding one year. Most patients had elevated PTH level and disordered calcium-phosphorus metabolism. Reported gastrointestinal manifestations were diverse, including upper and lower gastrointestinal bleeding, intestinal ischemic necrosis/ perforation, esophageal mucosal calcification, and colostomy fistula. Beyond gastrointestinal involvement, other vascular involvement manifestations primarily involved the skin (e.g., extremity gangrene, subcutaneous nodules, ischemic lesions), with some cases complicated by splenic infarction or penile calciphylaxis. Consistent with our findings, several reported cases showed that gastrointestinal manifestations preceded skin involvement or occurred in the absence of skin involvement. Treatment strategies included sodium thiosulfate, parathyroidectomy, surgical resection of the affected gastrointestinal tract, and proton pump inhibitors. Regarding outcomes, 4 patients survived, 6 died, and 2 were transferred to hospice care.