 Baseline characteristics of DITIN
Baseline characteristics of DITIN
A total of 6784 DITIN-related reports were included in the analysis. Of these, 3122 (46.0%) were from female patients and 3582 (52.8%) from male patients. By age, 3718 reports (54.8%) were from young and middle-aged individuals, and 3066 (45.2%) from elderly patients aged 65 years or older. The most common reported outcome was hospitalization, accounting for 3949 cases (58.2%), with 199 reports (2.9%) documenting death. The overall reporting trend showed a consistent increase over time (data not shown).
Drugs associated with TIN
Seventy-nine TIN-related drugs were identified (data not shown). The top 10 categories were as follows: antibacterial drugs (26/79), antineoplastic drugs (9/79), gastric acid secretion inhibitors (8/79), analgesic drugs (7/79), antihypertensive drugs (4/79), antiatherosclerotic drugs (4/79), antiepileptic drugs (3/79), immunomodulatory drugs (3/79), diuretic drugs (3/79), and antituberculosis drugs (2/79).
Suspected drugs for TIN
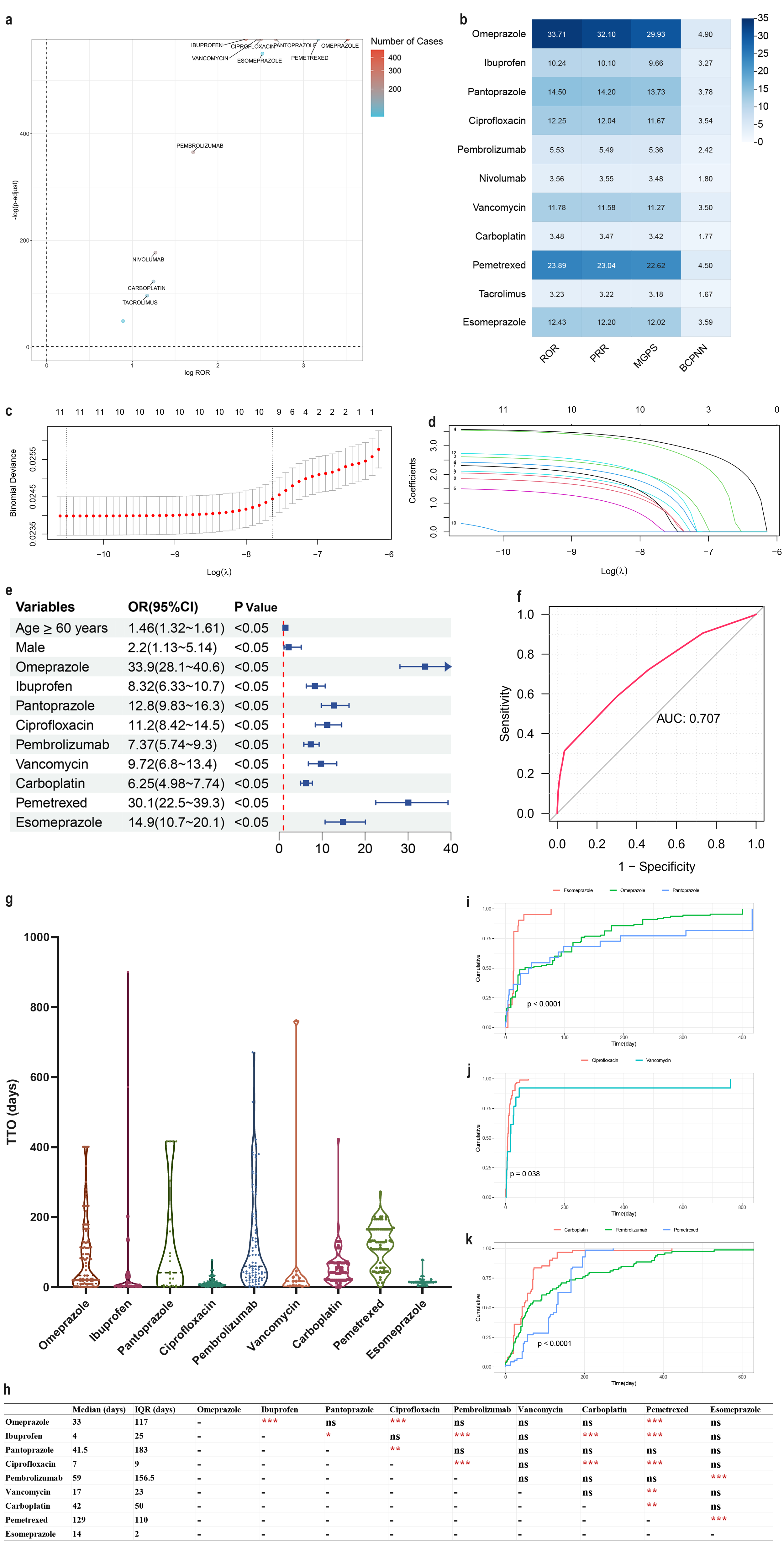
Drugs meeting the criteria of >100 case reports, a lower 95% confidence interval (CI) of the reporting odds ratio (ROR) >1, and adjusted p<0.01 were extracted for univariate analysis. As shown in Figure 1a, 11 such drugs were identified: omeprazole, ibuprofen, pantoprazole, ciprofloxacin, pembrolizumab, nivolumab, vancomycin, carboplatin, pemetrexed, tacrolimus, and esomeprazole.
The relationship between TIN and these suspected drugs is illustrated in the volcano plot (Figure 1a). In this plot, the x-axis represents the logarithm of ROR; a positive x-value indicates more frequent reporting of drug-related TIN compared with other adverse reactions. The y-axis represents the negative logarithm of the adjusted p-value (after Fisher’s exact test and Bonferroni correction), with a positive y-value denoting a highly significant difference. The color of each dot corresponds to the logarithm of the number of case reports, with redder shades indicating a higher number of reports. Thus, drugs located in the upper right quadrant of the plot exhibit both strong signal strength and significant differences. The thresholds of four data mining algorithms for these 11 drugs are shown in Figure 1b.
Risk factors for DITIN
LASSO regression analysis was performed on drugs with p<0.01 in the univariate analysis, yielding 9 candidate drugs (Figures 1c, 1d). Multivariate logistic regression analysis incorporating patient gender and age was then conducted (Figure 1e). The results indicated that male sex, age ≥60 years, and 9 drugs (omeprazole, ibuprofen, pantoprazole, ciprofloxacin, pembrolizumab, vancomycin, carboplatin, pemetrexed, and esomeprazole) were independent risk factors for DITIN. The model’s predictive accuracy, as measured by ROC-AUC, was 0.71 (Figure 1f).
Time interval from drug administration to TIN onset
The time interval from drug administration to TIN onset was evaluated (Figure 1g). The median onset time for TIN associated with the 9 drugs ranged from 4 days (fastest) to 129 days (slowest), with statistical differences detailed in Figure 1h. Further subgroup analyses of drugs within the same category (Figure 1i-k) showed that approximately 50% of reported cases among the 3 gastric acid secretion inhibitors occurred within 50 days of administration; ~90% of cases among the 2 antibacterial drugs occurred within 20 days; and ~75% of cases among the 3 antineoplastic drugs occurred within 200 days.
