A very young girl (15 years old) presented with generalized oedema and anuria for 2 days and confusion. On examination , GCS 3/15, BP-160/100 mmHg, PR-96/min, Heart – S1+S2+0, lungs- VBS with bibasal crepts, Abd- abdominal wall oedema, bilateral leg oedema (+), extensor plantar response on the left side . Urgent CT revealed acute infarct at right parietal lobe.
Urgent investigations revealed HBsAg, HCV Ab and HIV Ab- all clear, Urea – 31.32 mmol/L, Creatinine-1226 umol/L , Na-132, K-5.7, HCO3-19 , serum albumin- 23 g/dl, Hb-9.2 , WBC- 12.16 , Platelet – 285.
Urgent hemodialysis was started with right IJV temporary HD sheath.
After first time hemodialysis, she got fully concious with GCS 15/15) and her vital signs were stable and urine was coming out.
ANA – 1:80 (Speckled pattern, Trace), ENA profile – All Negative,
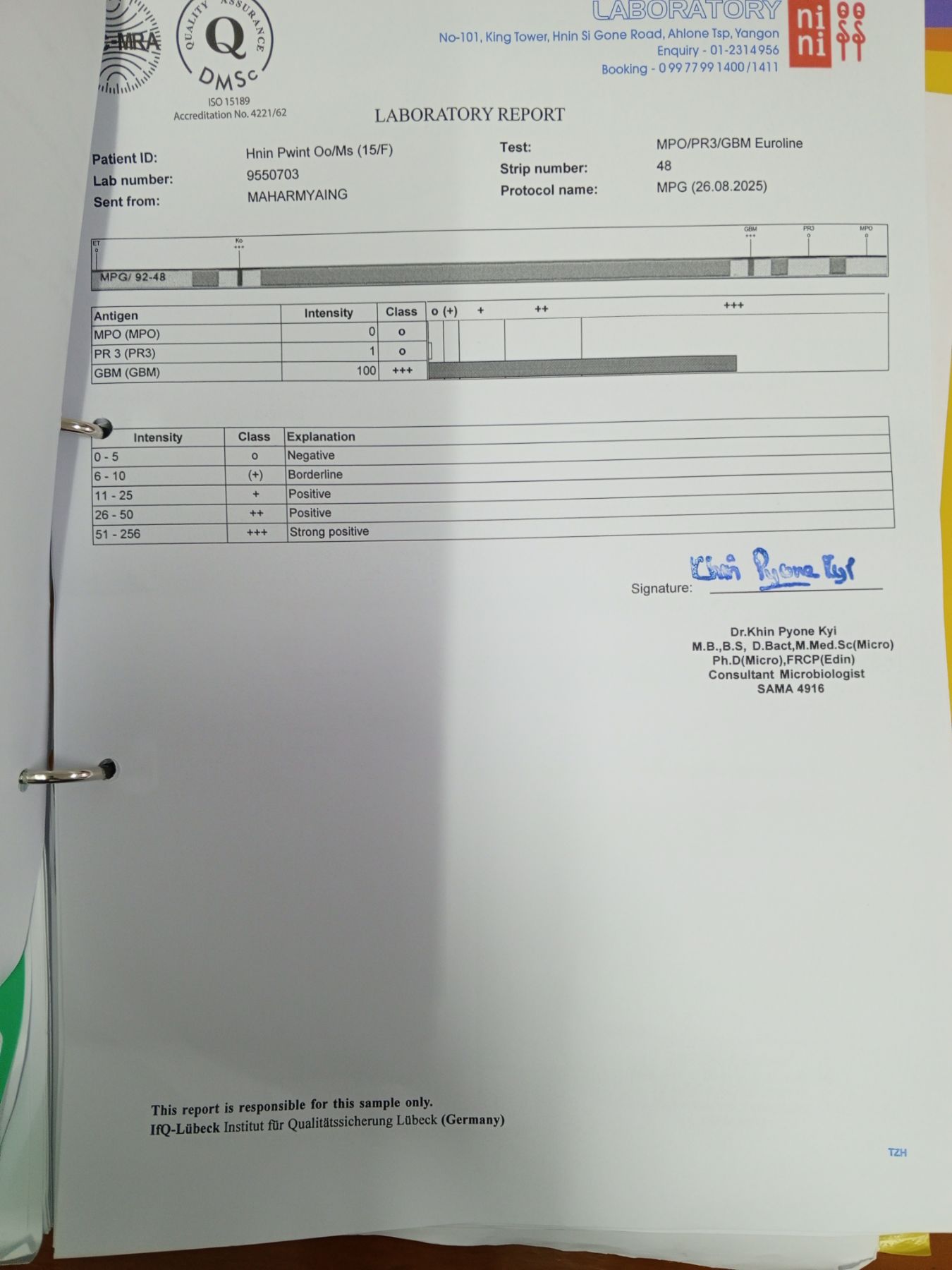
Anti PR3 – Negative, Anti MPO -Negative, Anti GBM (storongly Positive)- (+++) .
USG (abd) revealed right kidney – 9.37 cm with cortical thickness – 1.7cm , Left Kidney -10.85 cm with cortical thickness 1.62 cm, Ascites (++) and bilateral pleural effusion and stomach wall oedema.
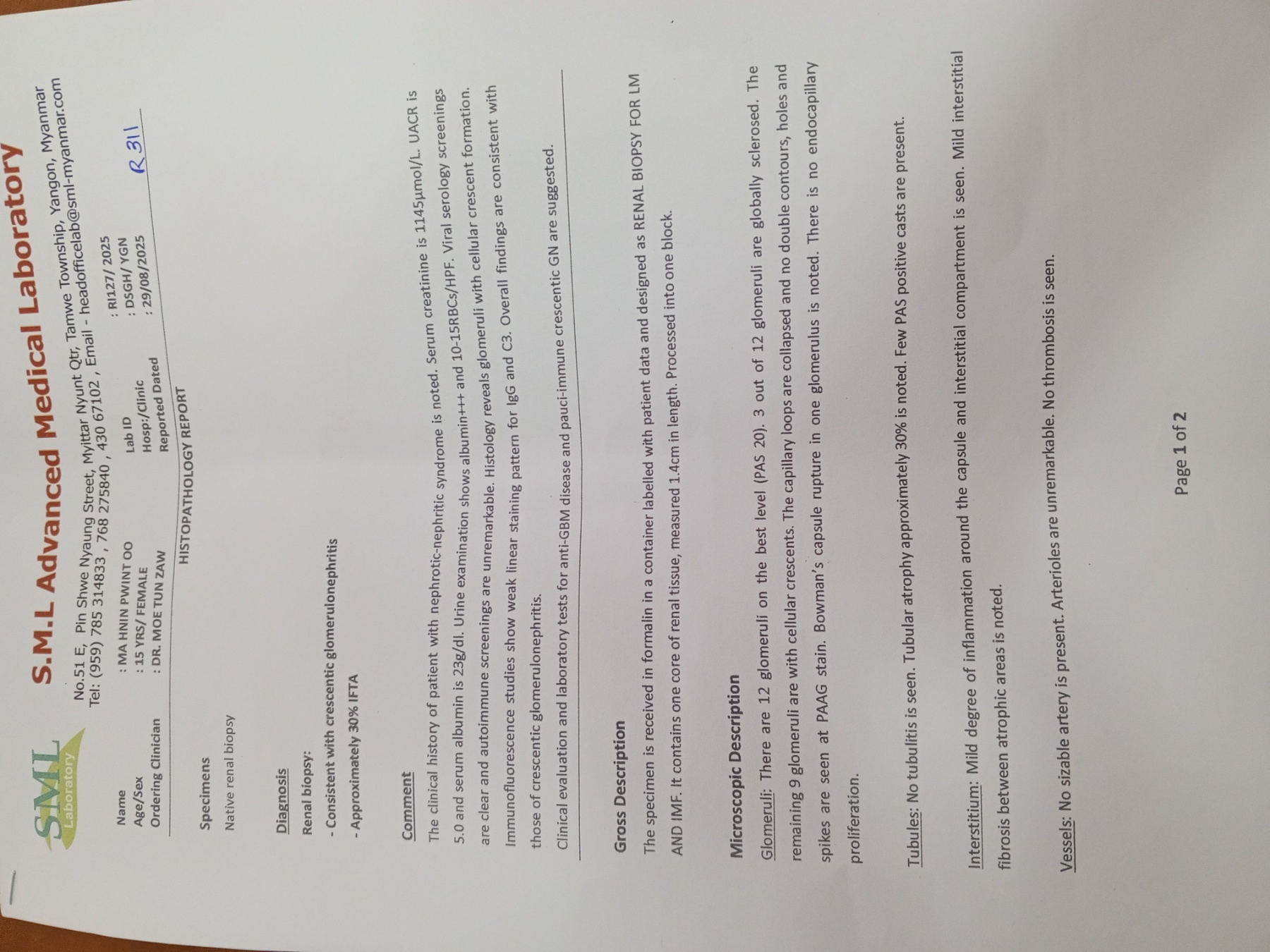
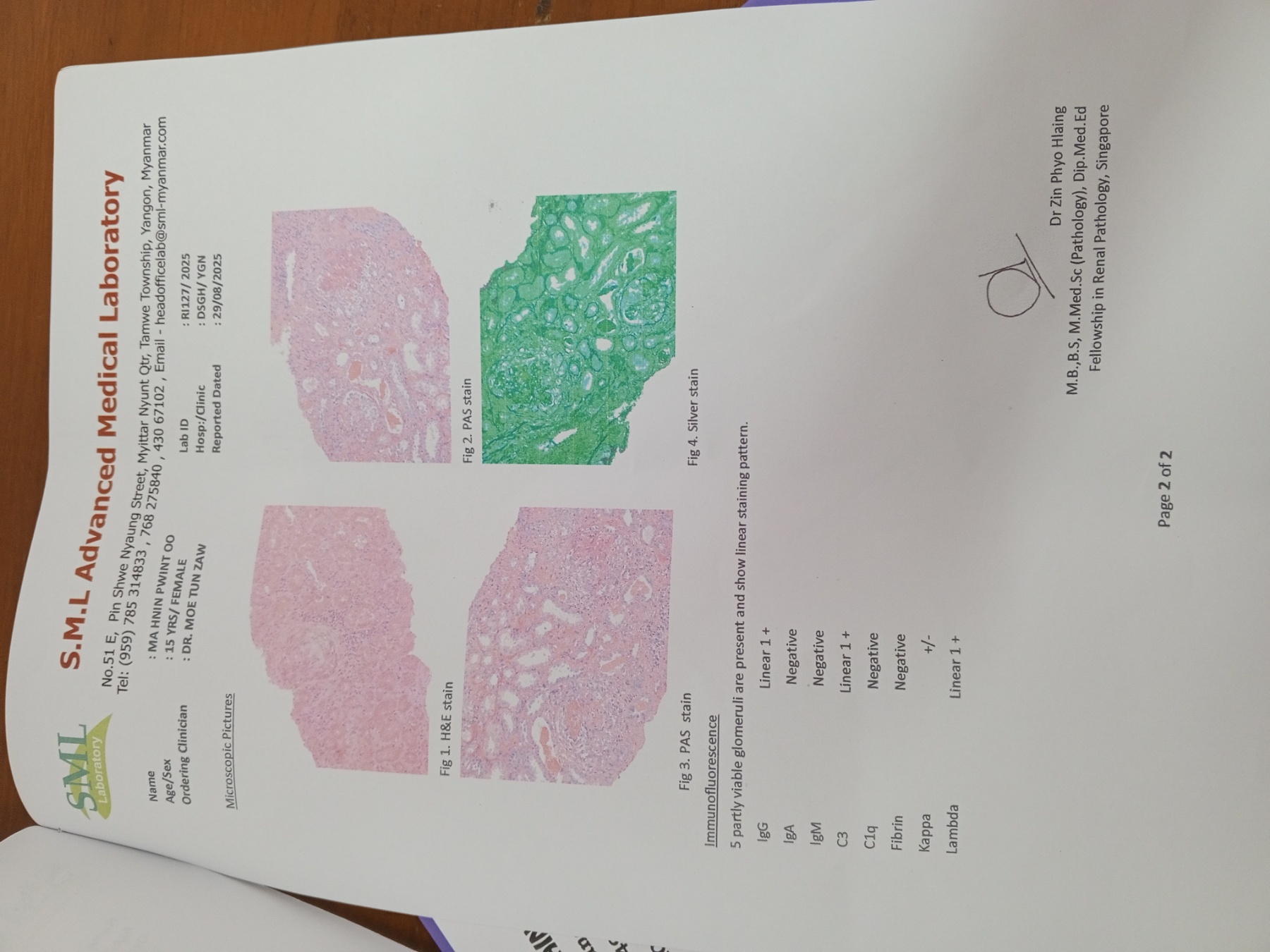
After 3 sessions of hemodialysis , her urea level-14.55 mmol/L and creatinine-554 umol/L and renal biopsy was done with 18 G renal biopsy gun , getting 12 glomeruli , 3 out of 12 glomeruli were globally sclerosed, the remaining 9 glomeruli were with cellular crescents, IF/TA – 30 % on light microscope and Immunoflourescence microscope showing 5 partly viable glomeruli are present and show linear staining pattern (IgG Linear 1+, IgA Negative, IgM Negative, C3 Linear 1 + , C1q Negative , Fibrin Negative, Kappa +/- , Lambda Linear 1+.
After getting renal biopsy result, IV pulse methylprednisolone 500mg+ N/S 100 ml was given for 3 days followed by oral prednisolone and IV cyclophosphamide (weight based renal friendly dosage)7.5mg/kg (IV Cyclophosphamide 300 mg + N/S 500 ml ) was given. She was planned to give 2 weekly IV cyclophosphamide for 6 dosages with the hope of dialysis independent in the future. Now she was on three times per week of maintenance hemodialysis.