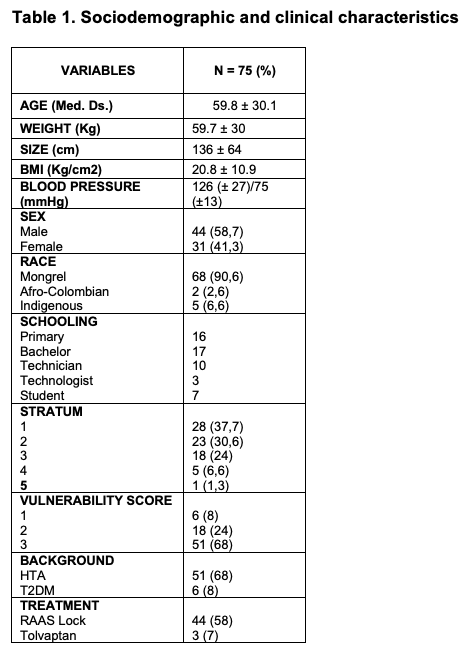
A study was conducted in 75 patients with polycystic kidney disease to explore the correlation between this pathology and social vulnerability. The sample was composed mostly of individuals of mestizo ethnicity (90.7%), with male predominance (58.7%) and a high concentration in low socioeconomic strata (37.3% in stratum 1). The social vulnerability score showed that 68% of the subjects had a high level of vulnerability, category 3 (greater vulnerability). Clinical variables such as arterial hypertension were found in (68%), type 2 diabetes mellitus (8%). see table 1.
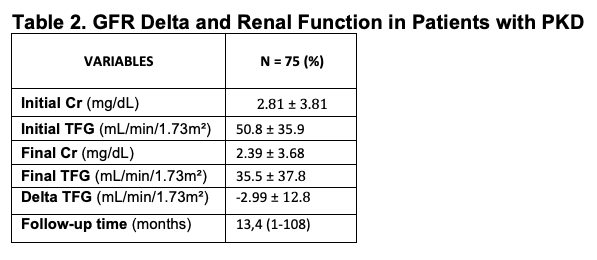
In descriptive analyses, the mean glomerular filtration rate at the beginning of follow-up was 50.8 mL/min/1.73m², decreasing on average 2.99 mL/min/1.73m² during the period analyzed. The group showed a high prevalence of arterial hypertension (68%) and symptoms associated with the disease (70.7%). The average initial creatinine was 2.81 and the final creatinine was 2.29, other data are shown in Table 2.
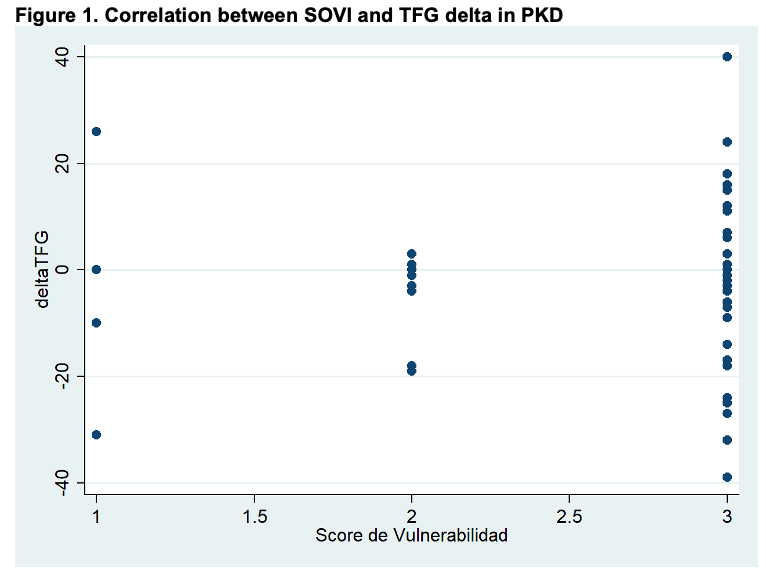
The correlation between the social vulnerability score and the glomerular filtration rate (IA) delta was evaluated using Spearman's correlation coefficient, resulting in a coefficient rho=0.0596 with a value p=0.6114, indicating that there is no statistically significant correlation between social vulnerability and the progression of kidney damage measured as a change in GFR in this cohort. See graph 1.
Analysis and discussion
PKD is a multi-organ disease whose determining factors in progression include genetic aspects (mutations in PKD1, PKD2) and clinical aspects (blood pressure control, use of RAAS blockers, presence of comorbidities)(15). This study provides evidence that social vulnerability, although elevated in most patients, is not significantly associated with the acceleration of kidney damage as measured by the decrease in GFR. This may be explained by the fact that the vulnerability score used may not capture social factors that directly impact renal function, or that other clinical variables have a greater weight on the progression of ERP. Previous studies indicate that the control of cardiovascular and genetic risks is more decisive in renal evolution than isolated social variables (Chebib & Torres, 2018; Cornec-Le Gall et al., 2019)(16)(17). However, the high prevalence of social vulnerability reflects the need for comprehensive care, considering social determinants that may affect adherence and quality of life (Musso et al., 2024)(11).
In addition, the presence of hypertension in 68% of the sample, a recognized factor for the worsening of ERP, emphasizes the importance of clinical management to slow progression. There may be indirect effects of social vulnerability on the control of these conditions that are not evident in this analysis with delta GFR in the short term.
Most of the patients analyzed presented high social vulnerability. Although a slight average decrease in GFR was observed, the correlation between the vulnerability score and the variation in glomerular filtration rate was not significant. The results suggest that additional factors, such as blood pressure control, use of RAAS blockers or tolvaptan, could influence progression.
The lack of significant correlation between social vulnerability and change in kidney function suggests that, in this sample, social vulnerability is not directly related to the measurable progression of polycystic kidney disease. It is possible that other clinical or genetic factors have a greater weight in progression, or that the vulnerability score used does not adequately capture aspects that directly impact renal function.
Additional analyses including clinical, genetic, and treatment variables are needed to assess their impact on renal progression.
The high proportion of patients in low strata and with high vulnerability highlights the significant social burden faced by these patients, which could affect other aspects of their quality of life and adherence to treatment. A comprehensive approach combining medical care with social interventions to improve outcomes in patients with ERP is suggested.
