The
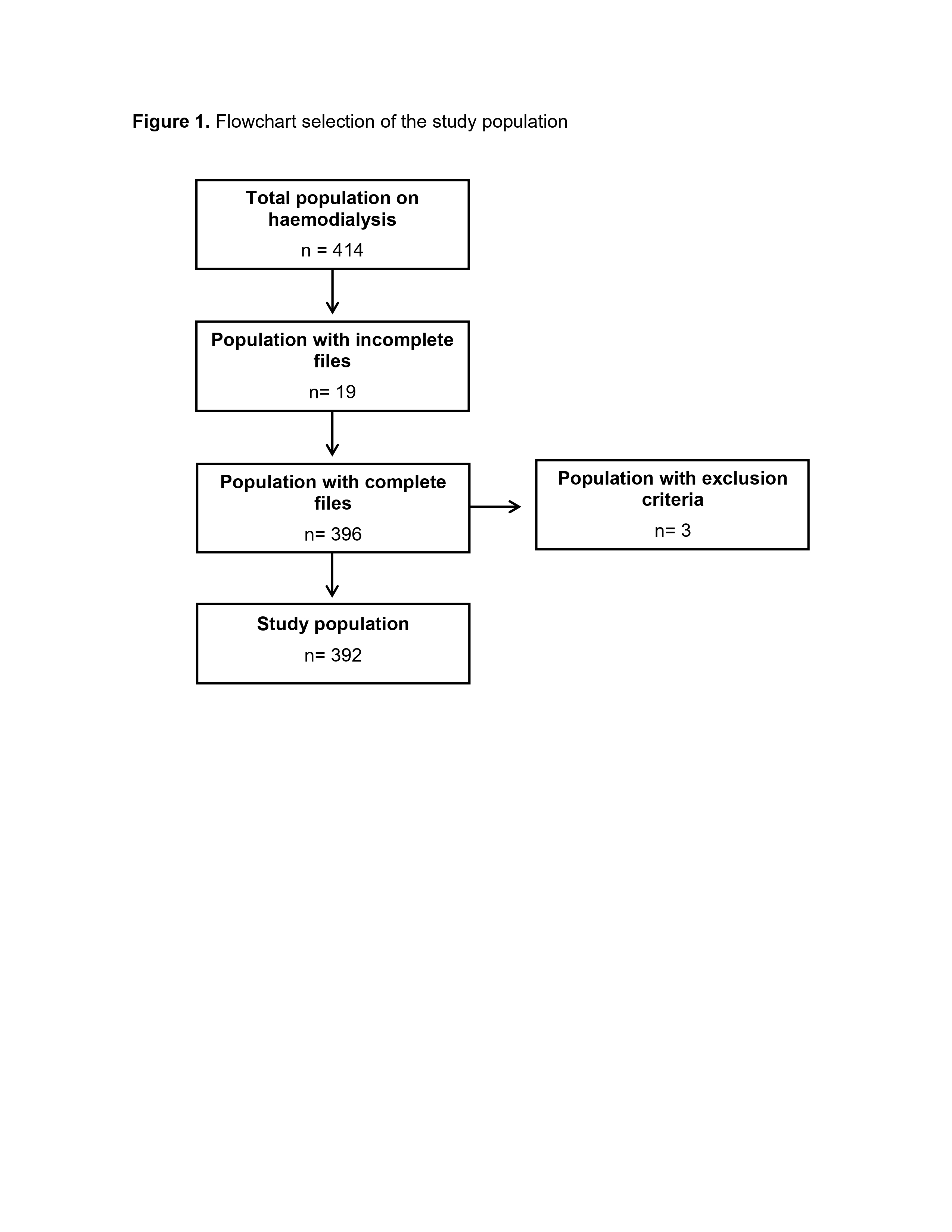
study population was obtained from the database of patients undergoing
hemodialysis therapy, from which a total of 414 medical records were
identified, of these, 392 met the eligibility criteria, while 21 were
excluded;19 because their records contained incomplete information and 3
because they were minors. Details of the selection process results are
presented in Figure 1.
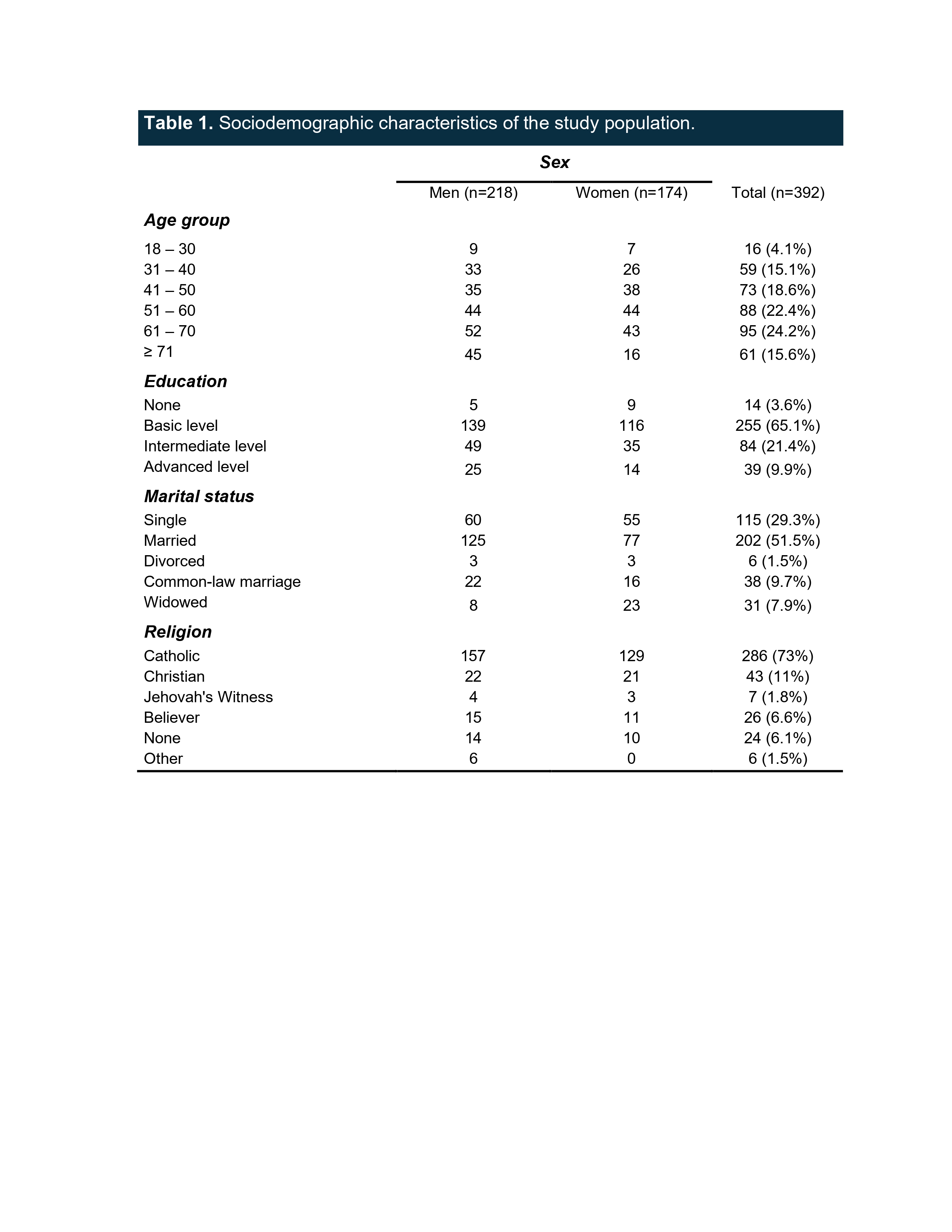
Regarding
the sociodemographic characteristics of the study population, 44.4% were women
and 55.6% were men. The mean age was 53 years with a standard deviation of
±14.6 years, with a median and mode of 57 years; there was wide variability by
age group, however, the 61-70 age group predominated with 24.2%. In terms of
educational level, basic education predominated with 65.1%; the most common
marital status was married with 51.5%; Catholicism was the predominant religion
with 73% of the population; the rest of the results are shown in Table 1.
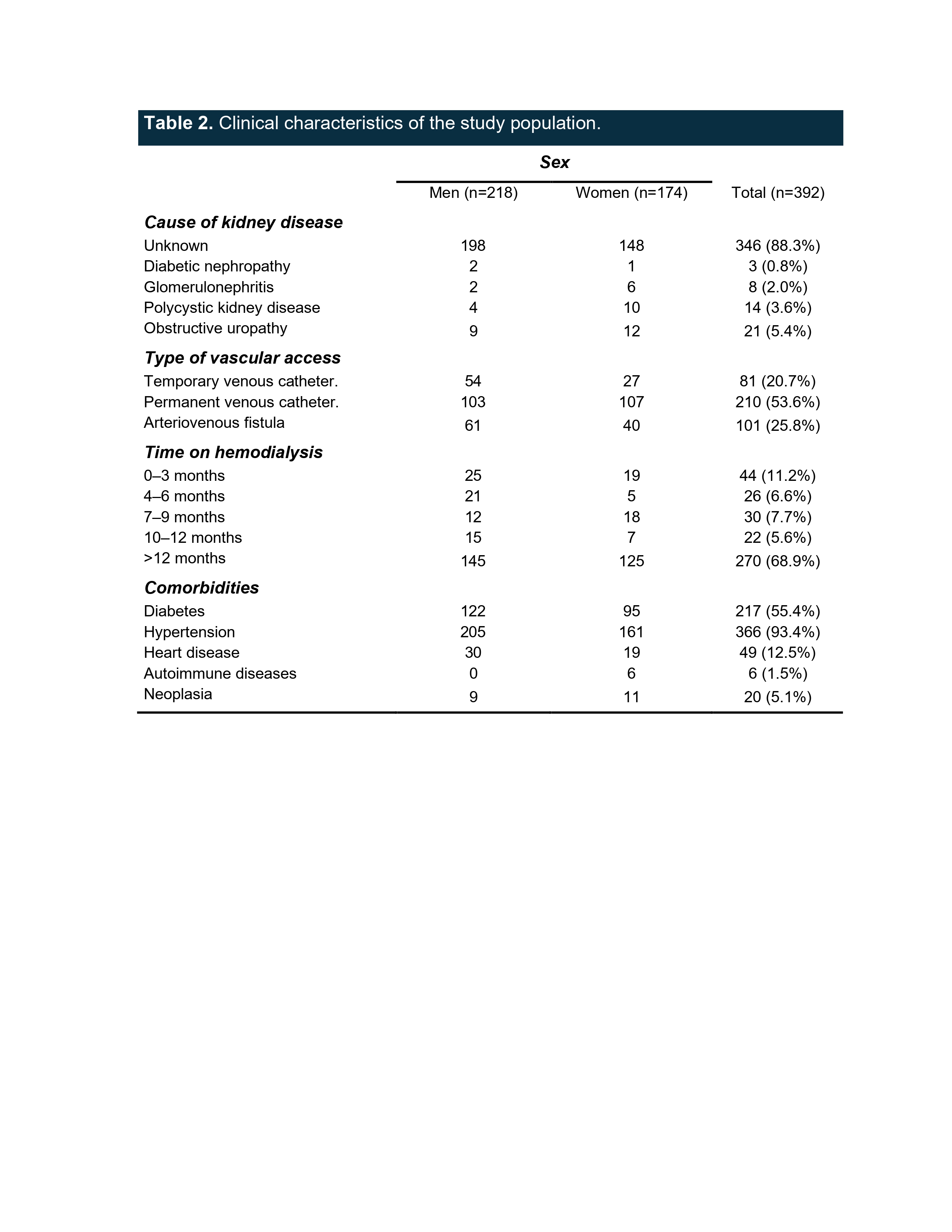
Table
2 shows the clinical characteristics of the study population, where the most
relevant finding was that the main etiology of kidney disease was unknown in
88.3% of cases. The predominant vascular access was a permanent catheter in
53.6% of cases, followed by arteriovenous fistula in 25.8% of cases, and
finally a temporary catheter in 20.7% of cases. It was found that 68.9% had
been on dialysis therapy for >12 months, and the main comorbidities reported
were hypertension in 93.4% and type 2 diabetes in 55.4%, with autoimmune
diseases being the least frequent at 1.5%.
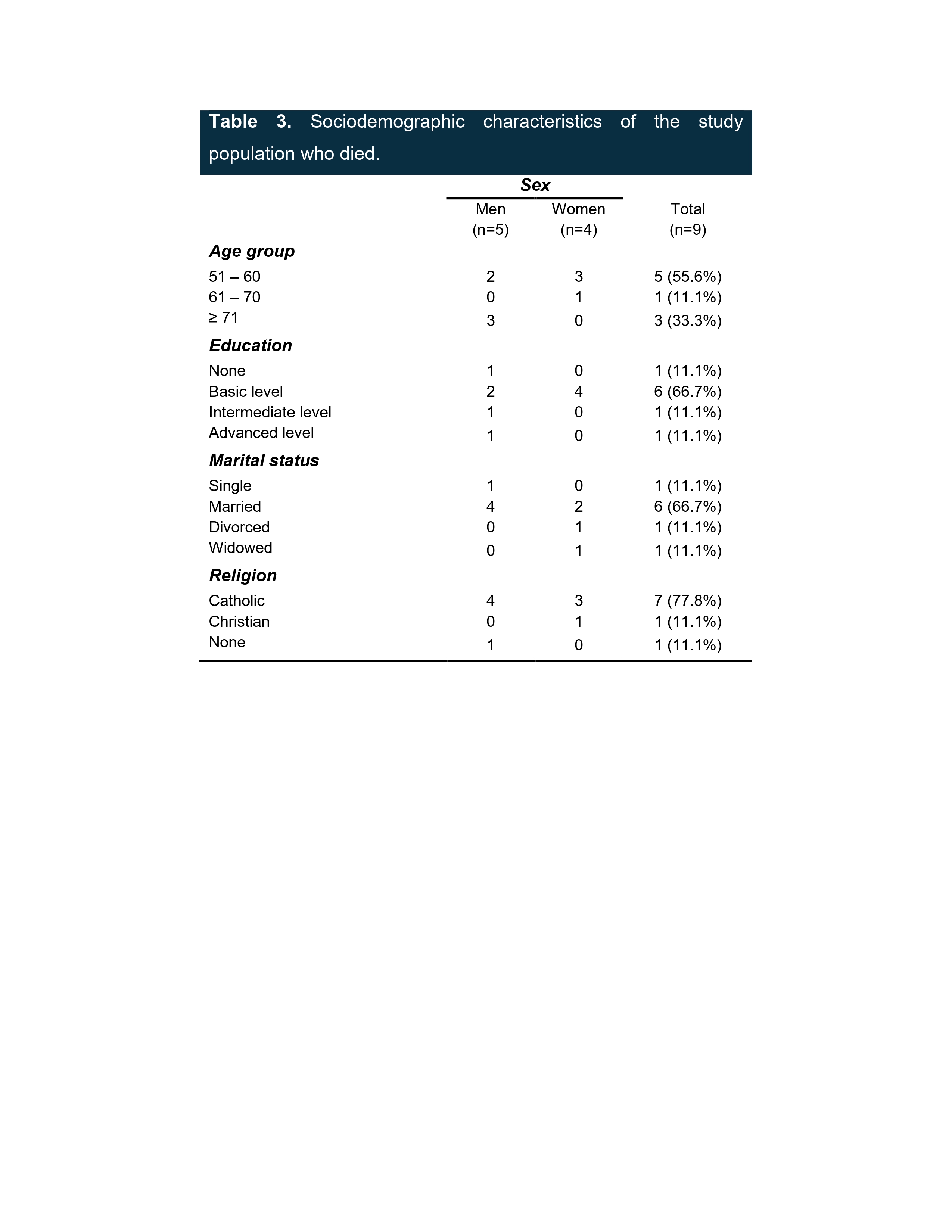
Of
the population studied, nine cases of patients who died during the study period
were identified, reporting that five men (55.6%) and four women (44.4%) died,
resulting in a mortality rate of 2.3% at the end of the study. The average age
was 63.4 years with a standard deviation of ±9.2 years, and the median and mode
of this variable was 59 years. Table 3 shows the sociodemographic
characteristics of this population, where it was documented that the
predominant educational level in the population that died was basic education,
at 66.7%.
In
terms of marital status, the majority of the deceased population was married
(66.7%), and the religion professed by the majority of the deceased population
was Catholic (77.8%).
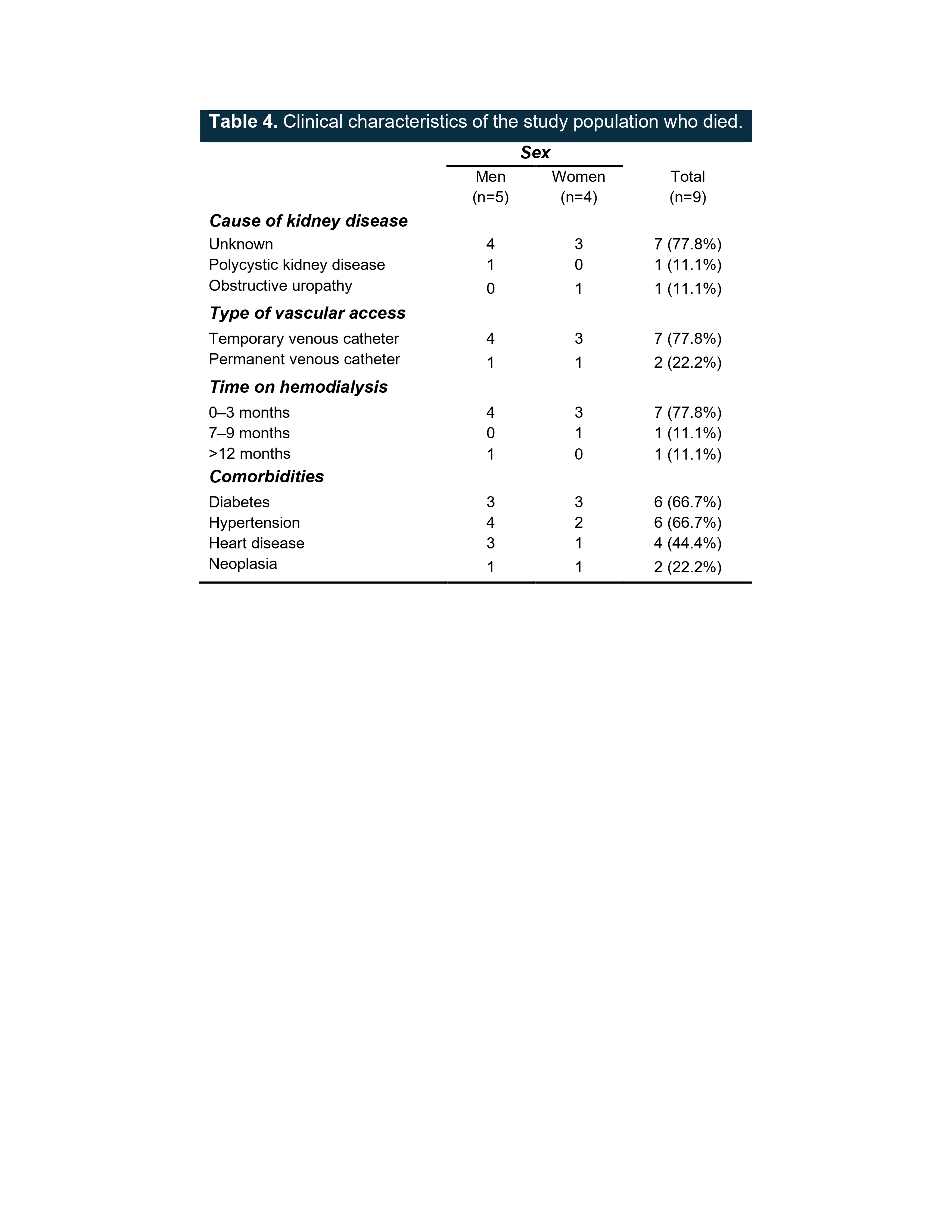
With
regard to the clinical characteristics (see Table 4) of the deceased
population, it was found that the main etiology of kidney disease was unknown
in 77.8%. Seventy-seven point eight percent used temporary vascular access and
22.2% used permanent vascular access; no deceased patients with arteriovenous
fistulas were identified.
Regarding
the duration of renal replacement therapy with hemodialysis, 77.8% had been on
dialysis therapy for 0-3 months. The most frequent comorbidities were
hypertension and diabetes, both with a prevalence of 66.7%, followed by
cardiovascular diseases with 44.4%. It was documented that 66.7% of the
deceased had two or more comorbidities, and two cases (22.2%) were documented
without any comorbidities.
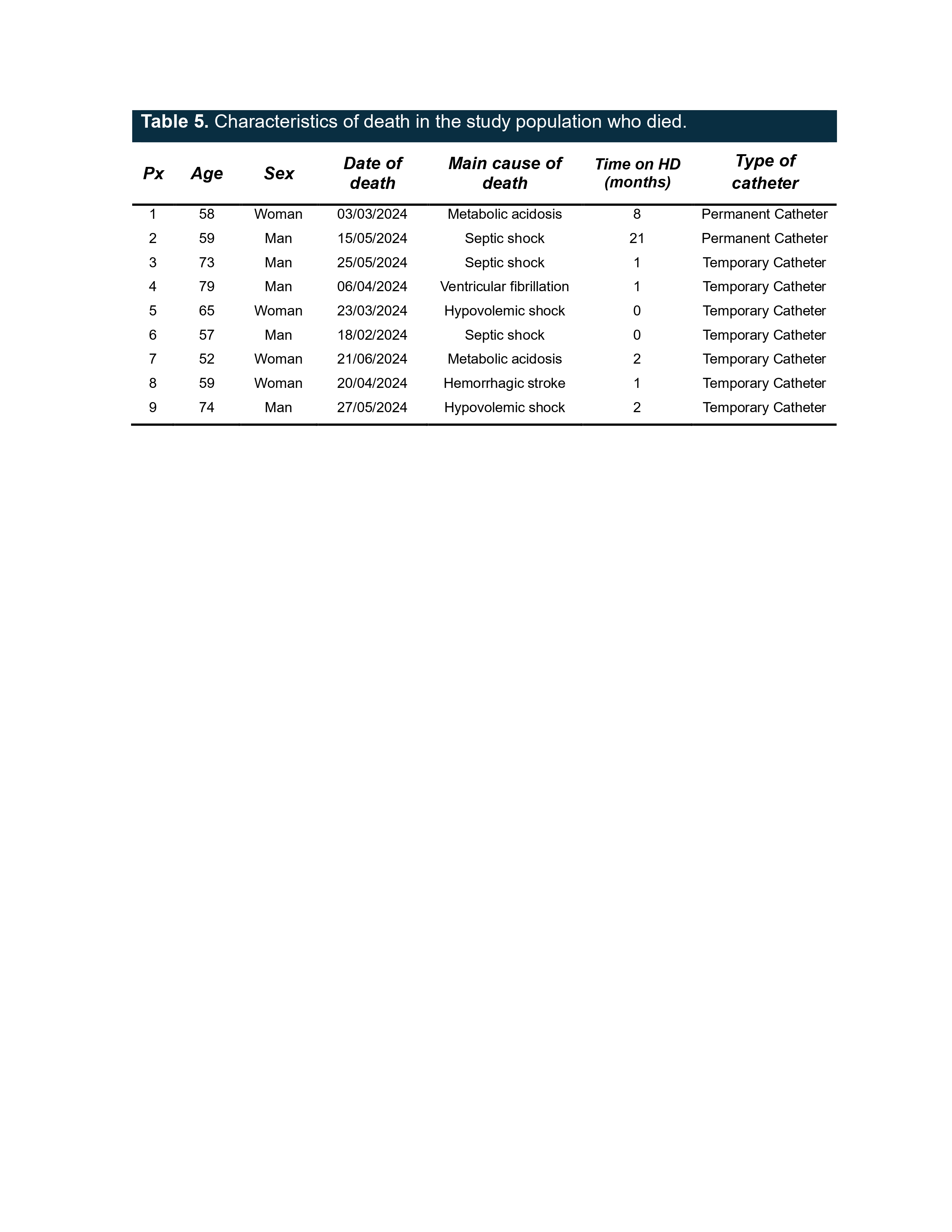
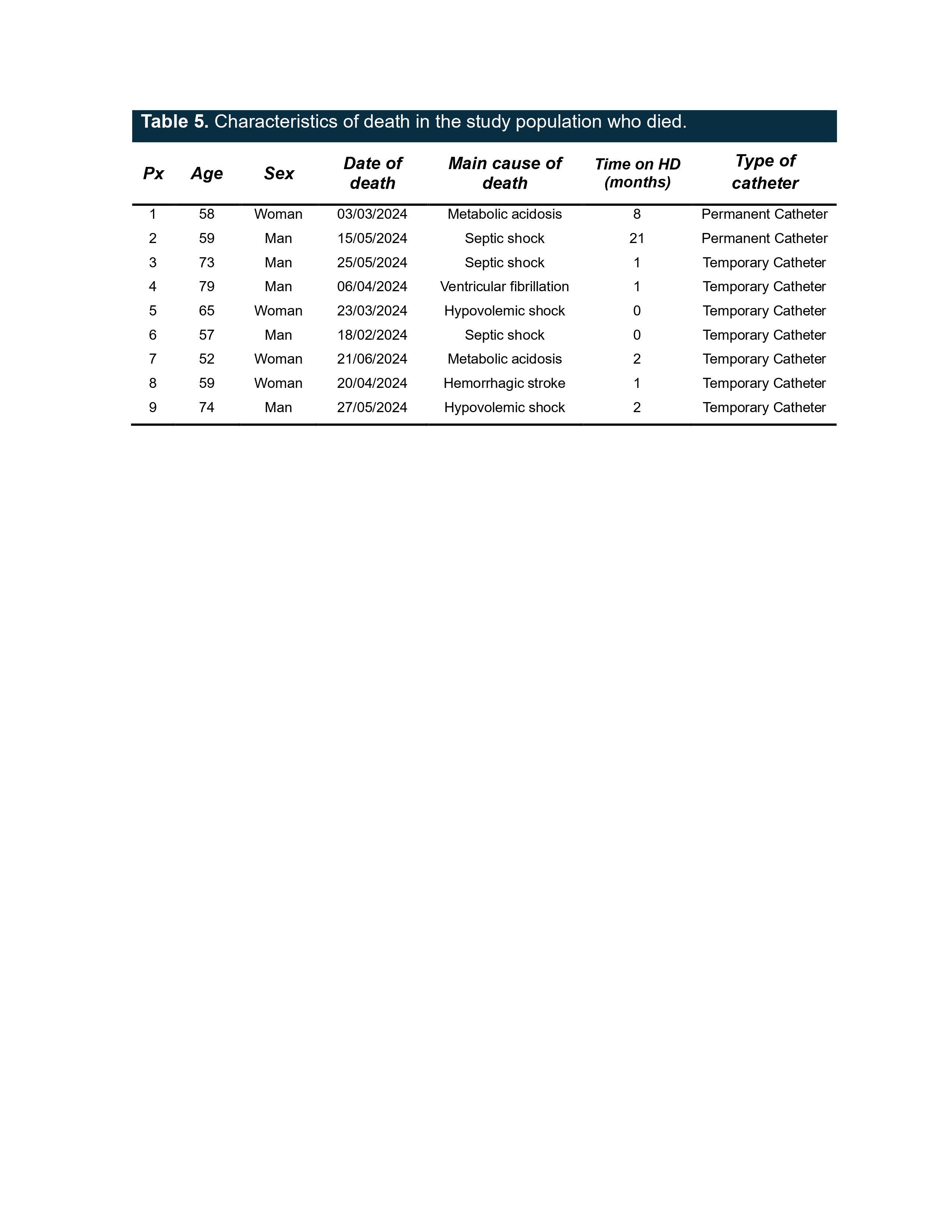
The
main causes of death were compiled, finding cardiovascular causes in 4 cases
(44.4%), infectious causes in 3 cases (33.3%), and metabolic causes in 2 cases
(22.2%) (see Table 5).
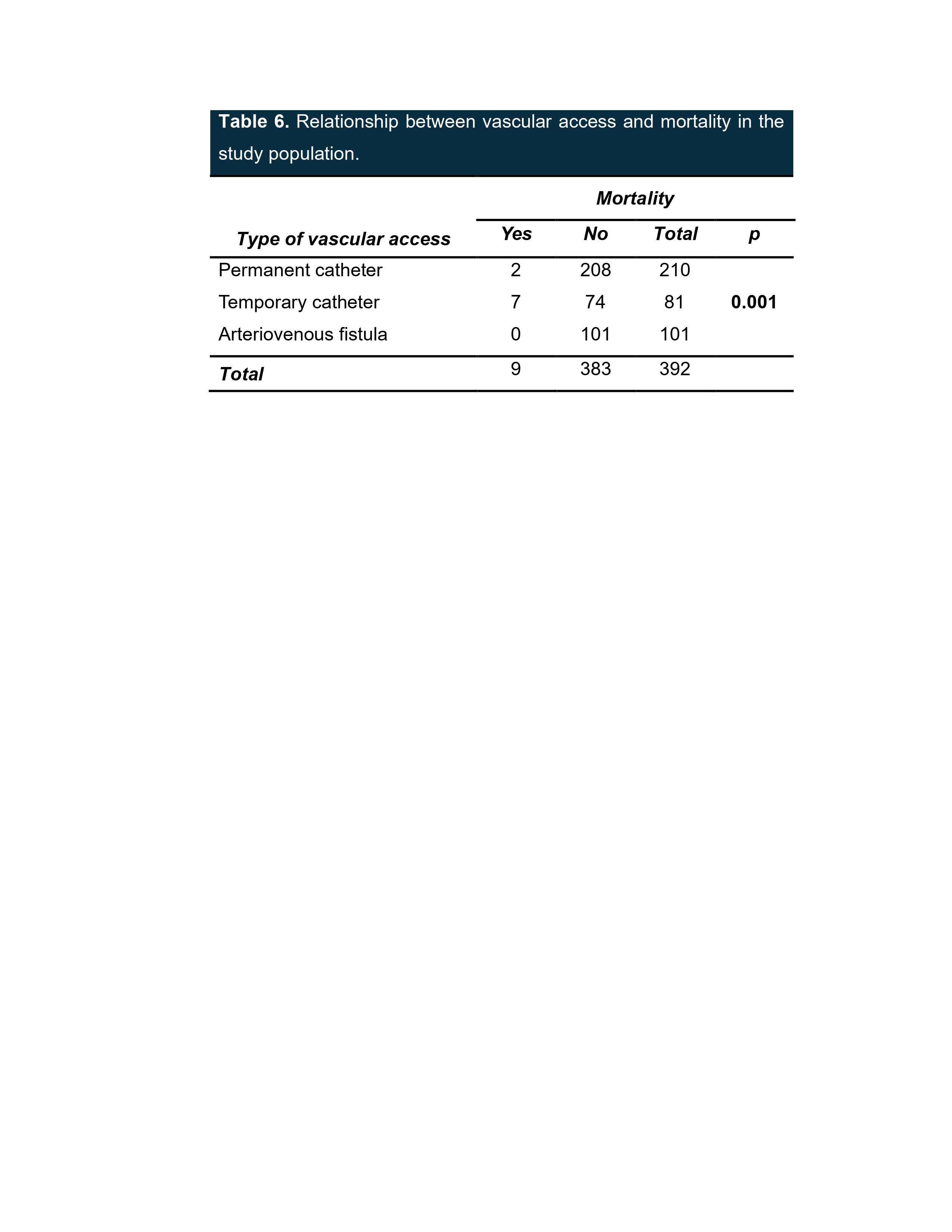
When performing the bivariate analysis, Fisher's exact test
was used to establish the relationship between the study variables. A
relationship was demonstrated between the type of vascular access and death,
obtaining a p-value of 0.001 (see Table 6).
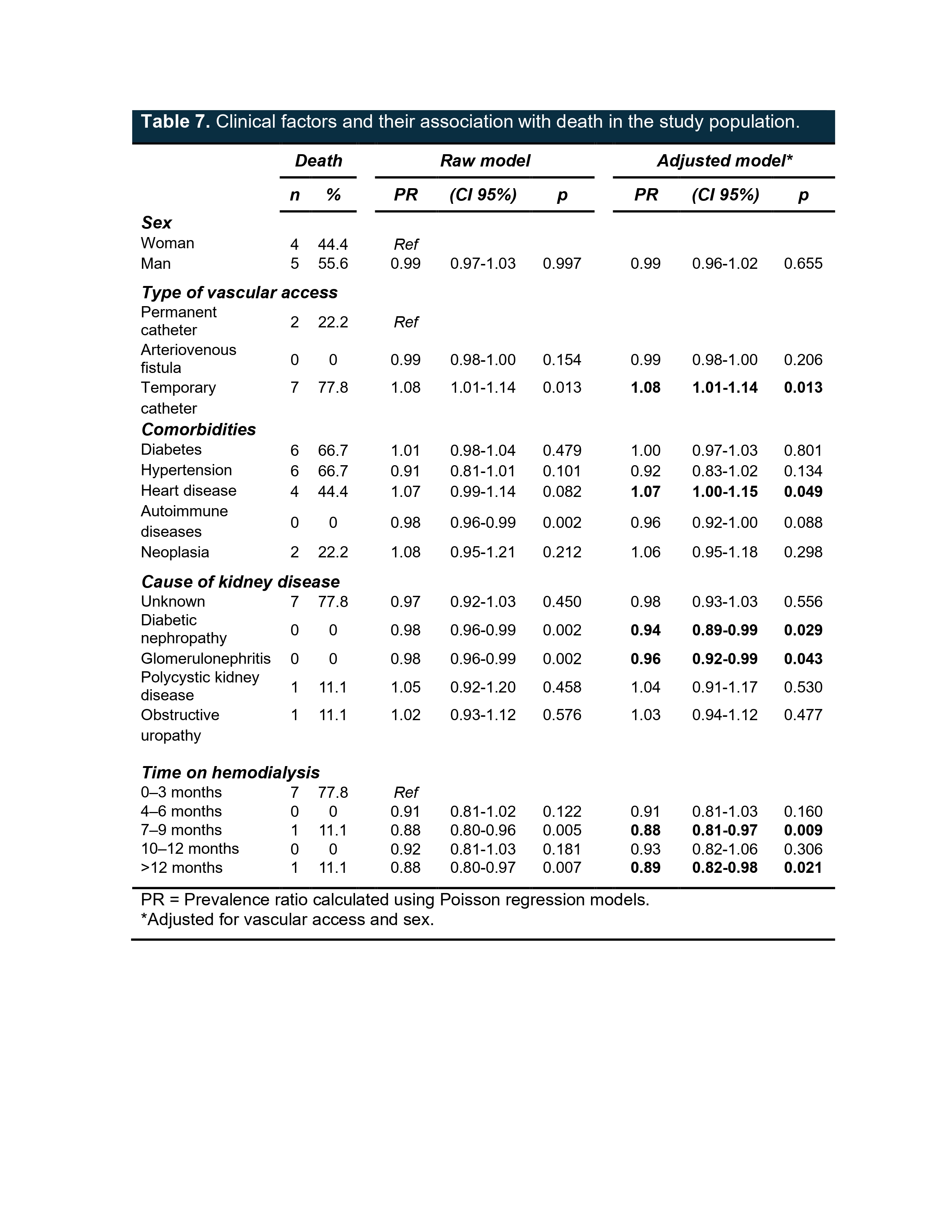
Poisson
regression was performed to observe the clinical factors associated with
mortality and the type of vascular access used. In the population with chronic
kidney disease undergoing hemodialysis replacement therapy at HGR C/MF No. 1,
the prevalence of death in those who had a temporary catheter was 8% (p=0.013)
compared to those with a permanent catheter, which was statistically
significant.
Similarly,
it was documented that there was a comorbidity associated with mortality, which
was heart disease, with a prevalence of 7% (p=0.049), which was statistically
significant. When
performing this regression, some protective factors were found, such as having
diabetic nephropathy as the etiology of kidney disease (p=0.029) and some
glomerulonephritis (p=0.043), as well as the duration of hemodialysis therapy
being 7 to 9 months (p=0.009) and >12 months (p=0.021) for those who showed
this behavior (see Table 7).
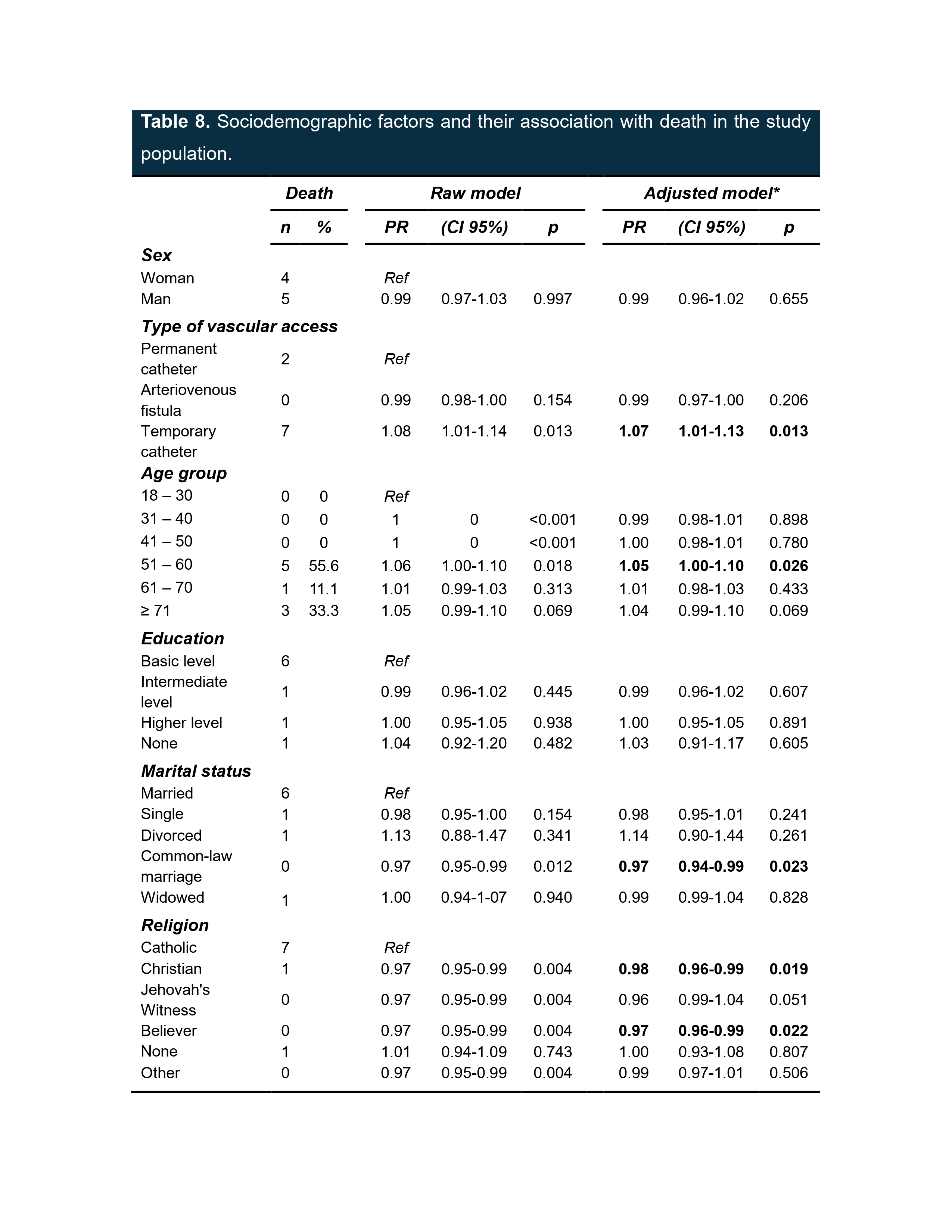
Similarly, Poisson regression
was performed to observe sociodemographic factors, and belonging to the 51-60
age group was found to be a risk factor for mortality, corresponding to a 5%
(p=0.026) risk and being statistically significant. As with clinical factors,
we found protective factors for mortality, including marital status, with
cohabitation providing this protection (p=0.023), as well as Catholic religion
(p=0.019), both of which were statistically significant (see Table 8).
STUDY LIMITATIONS
Although the sample size is large, our study is
still observational and can therefore only support inferences about
associations; confounding factors cannot be ruled out. Ideally, only a
randomized clinical trial assigning both access types could clarify whether the
relationship between access type and mortality is causal.
We recognize that our protocol also has some
limitations, such as the lack of analysis of other risk factors that could
impact mortality, some of which could be hemodialysis time, KT/V,
ultrafiltration in each hemodialysis session, psychosocial status, and
treatment adherence, among others.
FUTURE RESEARCH
For future research, we suggest considering the
inclusion of clinical, biochemical, and sociodemographic variables that have
been shown to be associated with mortality in hemodialysis patients, as well as
extending the study period and evaluating a clinical trial for greater control
of variables.
