The study
encompassed 578 incident HD patients (346M and 232F) with the average age 63,4±12,0 years and the average HD vintage 73,54±68,97 months, but 187 patients (96M and 91F) or 32,3% were with CVC as
vascular access for hemodialysis. Over the observed period 43 CRBSIs were
registered, 32 in 118 patients with TCVC (14465 catheter-days) and 11 in 69
patients with PCVC (17820 catheter-days), but 11 patients had multiple CRBSIs.
There was statistically significant difference of CRBSI rate between patients
with TCVC and PCVC (2,212 vs 0,617 CRBSI/1000 catheter-days respectively, Chi
square 15,267, p<0.001). Femoral site was in 60,5%, subclavian in 20,9% and
jugular in 18,6% of patients with CRBSI. The prevalent bacteria determined were
Staphylococcus coagulase negative in 27,9%, Staphylococcus aureus in 16,3% and
Methicillin resistant staphylococcus aureus-MRSA in 11,6% of CRBSIs. Patients
with CRBSI in comparison to patients without CRBSI had statistically
significant lower mean serum albumin (32,93±5,02 vs 37,09±3,61 g/L, p<0.001),
hemoglobin (94,69±14,87 vs 116,73±12,78 g/L, p<0.001) and higher CRP (39,29±43,39
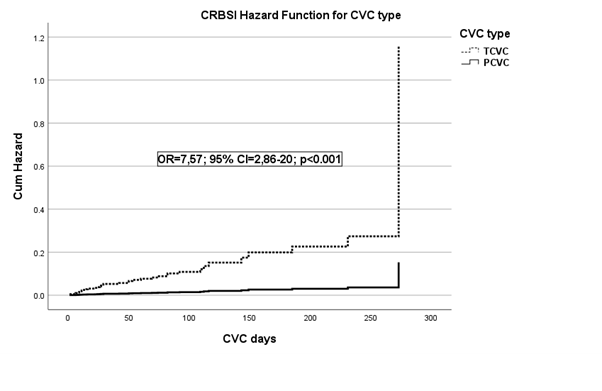
vs 11,94±25,58 mg/L, p<0.001). Cox regression analysis showed that the model
was statistically significant (Chi square 96,54; df=6; p<0.001) and statistically
significant risk factors for CRBSI were TCVC type in comparison to PCVC (OR=7,57;
95% CI=2,86-20,0; p<0.001), hemoglobin <100 g/L in comparison to Hgb ≥100 g/L (OR=6,75; 95%
CI=3,45-13,15; p<0.001), serum albumin <35 g/L in comparison to
albumin ≥35 g/L (OR= 2,48; 95% CI=1,30-4,74; p=0.006), and CRP ≥6 mg/L in
comparison to CRP <6 mg/L (OR=5,14; 95% CI=1,55-17,07; p=0.007). Age,
gender, HD duration, DM, and CVC site were not significant risk factors for
CRBSI.