ECG showed tachycardia and shortened QT. A provisional
diagnosis of Acute pancreatitis was made and she was started on IV Antibiotics,
IV Fluids, anti-convulsants and other supportive measures. Her chest radiographs revealed ARDS
and she was put on Non-Invasive ventilation. Her labs showed elevated total count of 15,000 cells/µL, Hemoglobin of
14g/dl, hypokalemia (2.9 mmol/l), hypernatremia (147 mmol/l), elevated renal
parameters (blood urea 49 - mg/dl, serum creatinine – 1.6 mg/dl), total
bilirubin (3.2 mg/dl) and unconjugated bilirubin (1.8 mg/dl) with normal
transaminases and normal albumin (3.9g/dl). Her Serum amylase (524 U/l) and
serum Lipase (620 U/l) were elevated. Her Serum Calcium was very high (23mg/dl),
C-reactive protein (CRP) was elevated (69 U/l), vitamin D (51.1 ng/ml) was near normal while phosphorus
level was mildly elevated (5.37 mg/dl). ABG revealed severe metabolic alkalosis
with respiratory compensation. Her serum magnesium levels, Serum Lactate dehydrogenase (LDH), Troponin (Trop) I,
Serum triglycerides and coagulation
profile were in the normal range. In view of severe hypercalcemia, she was
started on IV steroids, subcutaneous calcitonin (200 U s/c bid), cinacalcet (30mg
bid) and volume expansion with fluids. Her urine output remained good during
the initial course of illness. Bisphosphonates were avoided in view of
exponentially rising renal parameters.
Serum intact Parathormone level was found to be
elevated (988 pg/ml). Her serum ACE level, CA 19-9 and CA-125 were normal. She
was screened for source of PTH and neck ultrasound revealed a nodule in right
lobe of thyroid gland inferiorly measuring 35x28x30mm with vascularity (Fig 1).
Her ultrasound showed normal sized kidneys with renal calculus (5mm) in upper pole of left
kidney (Fig. 2). Contrast CT Abdomen was suggestive of bulky pancreas with CT
severity score of 4/10, consolidation in bilateral basal zone of lungs with
minimal left pleural effusion, bilateral non obstructive renal calculi, mild
ascites, umbilical hernia, neck screening showed nodule in right inferior lobe of
thyroid gland. FNAC of gland showed small round cells with smooth nuclear
borders, dark nucleoli, salt and pepper chromatin with eosinophilic cytoplasm
with inflammatory and hemorrhagic background. Her Technitium (Tc)99m sestamibi parathyroid
scan (Fig 3) showed abnormal focal tracer uptake in inferior lobe of right
thyroid.
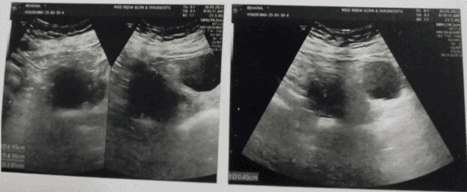
Fig. 1 Ultrasound of neck showing parathyroid adenoma in right inferior thyroid lobe.
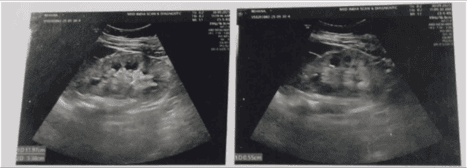
Fig. 2 Ultrasound of kidneys showing left kidney upper pole renal calculus.
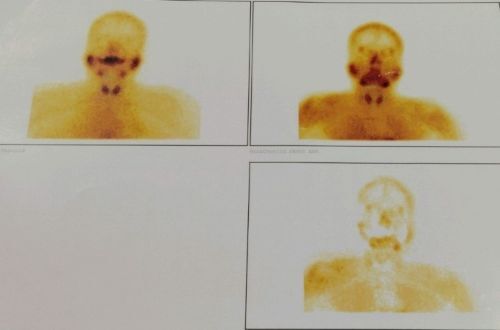
Fig.3 Technitium (Tc) 99m Sestamibi Parathyroid scintigraphy
scan suggestive of functioning parathyroid adenoma with no tracer uptake post
parathyroidectomy.
In view of worsening renal function, oligo-anuria,
pulmonary oedema and persistently elevated serum calcium level, she underwent 1
session of hemodialysis with a high flux dialyzer through the right femoral uncuffed double lumen dialysis catheter with a low calcium dialysate bath. She
improved well with serum calcium levels dip from 20mg/dl to 15mg/dl then 9.5 mg/dl. She underwent parathyroidectomy after preoperative
assessment and clearance for surgery and the Histopathological examination(HPE) of gland showed nuclear
pleomorphism with condensed chromatin with fibrous septation, thick-walled
vessels with areas of hemorrhage suggesting parathyroid adenoma. She improved over the course of treatment with
normalization of renal functions, urine output, serum calcium (8.5mg/dl), serum
amylase (71 U/l) lipase (106 U/l), PTH (195 pg/ml). She was diagnosed as severe
hypercalcemia due to PHPT secondary to functioning parathyroid adenoma with
acute pancreatitis, renal calculus, seizure and acute kidney injury needing
dialysis for control of hypercalcemic crisis, recovering post parathyroidectomy. She was discharged in a stable condition condition with advised treatment
and follow up.
