Of 4105 AKI cases, 160 were PRAKI (3.9%). Among approximately
47,059 deliveries, the incidence of PRAKI was 0.34%. The study included a total of 200
pregnant women with a mean age of 30.8 ± 8.0 years (range 18–44 years). The
largest proportion of participants were in the 18–27 years age group (39%),
followed by 28–37 years (33%) and 38–47 years (28%).
Table 1: Socio demographic
Characteristics of Pregnant Women with Acute Kidney Injury
|
Base line
|
Frequency
|
Percent
|
|
Age
|
18-27 years
|
88
|
44.0
|
|
28-37 years
|
76
|
38.0
|
|
38-47 years
|
36
|
18.0
|
|
Parity
|
Multi gravida
|
107
|
53.5
|
|
Primi gravida
|
93
|
46.5
|
The study included a total of 200 pregnant women with a mean
age of 30.8 ± 8.0 years (range 18–44 years). The largest proportion of
participants were in the 18–27 years age group (44%), followed by 28–37 years
(38%) and 38–47 years (18%). With respect to parity, a slightly higher
proportion were multigravida (53.5%) compared to primigravida (46.5%).
Table 2: Obstetric Profile
|
Variable
|
Category
|
Frequency
|
Percent
|
|
Trimester
|
1st trimester
|
49
|
24.5
|
|
2nd trimester
|
75
|
32.5
|
|
3rd trimester
|
86
|
43
|
|
Mode
of delivery
|
Normal vaginal
delivery
|
62
|
31
|
|
Cesarean section
|
51
|
25.5
|
|
Preterm/Assisted*
|
44
|
22
|
|
Undelivered/Other
outcome*
|
43
|
21.5
|
|
ANC
check-up
|
Yes
|
108
|
54
|
|
No
|
92
|
46
|
Majority were in the
3rd trimester (43%), followed
by the 2nd trimester (32.5%) and the 1st trimester
(24.5%). . Regarding delivery outcomes,
31% had a normal vaginal delivery and 25.5% underwent cesarean section, whereas
22% had preterm or assisted deliveries and 21.5% were undelivered or had other
outcomes at the time of assessment. More than half of the women (54%) had
undergone at least one antenatal check-up.
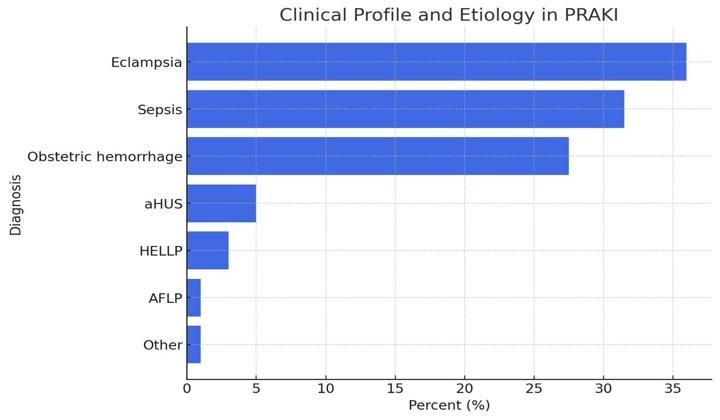
Table 3: Clinical Profile and Etiology
|
|
Frequency
|
Percent
|
|
Diagnosis
|
Eclampsia
|
72
|
36
|
|
Sepsis
|
63
|
31.5
|
|
Obstretric hemorrhage
|
45
|
27.5
|
|
aHUS
|
10
|
5
|
|
HELLP
|
6
|
3
|
|
AFLP
|
2
|
1
|
|
Other
|
2
|
1
|
History of hypertension disorder was present in 29% of pregnant
women with acute kidney injury (AKI), while 71% had no such history. At
presentation, 53.5% were hypertensive and 46.5% were normotensive.
Creatinine
at Presentation (Mean ± SD): 3.45 ± 2.59 mg/dL
Need for Hemodialysis: 40 (25.0%)
On dialysis during discharge- 10(5%)
Plasma Exchange (PLEX): 16 (10.0%)
The major etiologies of PRAKI were:
Preeclampsia/eclampsia
- 36%
Postpartum
hemorrhage – 31.5%
Sepsis – 27.5%
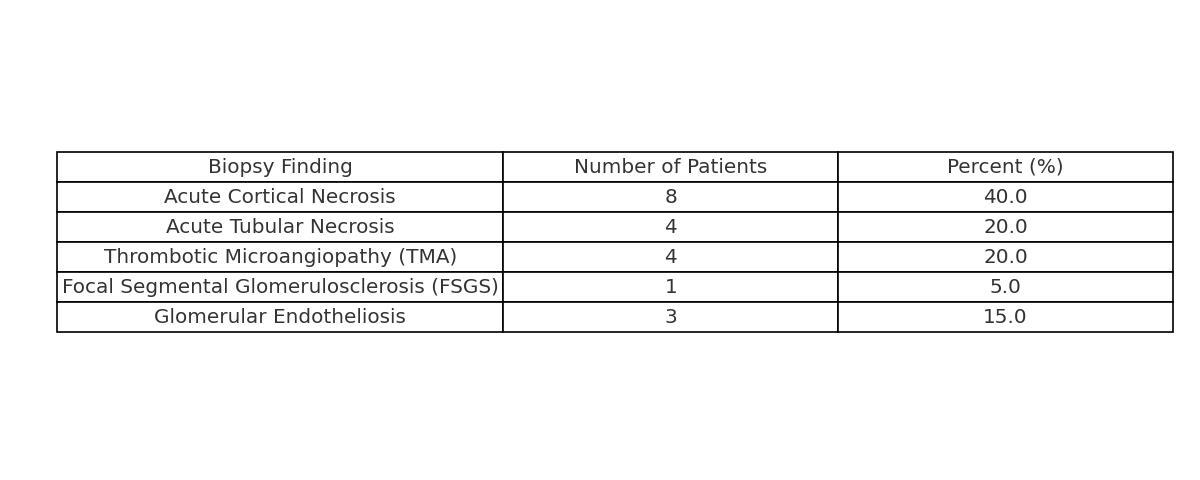
Biopsy was done in patients having persistent AKI beyond 6 weeks.
In terms of maternal outcomes, 53.5% of pregnant women with
acute kidney injury (AKI) died, while 46.5% survived. Regarding recovery
status, only 50% achieved complete recovery indicating residual renal
impairment. Fetal outcomes were similarly affected, with 48.5% of fetuses
surviving and 51.5% experiencing adverse outcomes.
The association between creatinine levels and maternal and fetal
outcomes was analyzed. Among patients with normal creatinine, 86% survived and
14% died, whereas among those with high creatinine ( more than 5mg/dl) 56.6%
survived and 44.4% died; this difference was not statistically significant (χ²
= 2.313, p = 0.128). For complete recovery, 86.2% of patients with normal
creatinine recovered completely compared to 13.8% of those with high creatinine
(χ² = 0.205, p = 0.651). Fetal recovery was significantly associated with
maternal creatinine levels. In the normal creatinine group, 88.2% of the
fetuses survived (0%), whereas in the high creatinine group, 49.7% of fetuses
survived and 50.3% did not. This difference was statistically significant (χ² =
4.829, p = 0.028). Hypertension status was not significantly associated with
creatinine levels, with 46.2% normotensive and 53.8% hypertensive among the
high creatinine group (χ² = 0.376, p = 0.540).
Our results highlight the significance of enhancing
multidisciplinary management including obstetrics, nephrology, and critical
care teams, as well as enhancing antenatal surveillance and guaranteeing prompt
referral to tertiary hospitals. PRAKI incidence and outcomes are anticipated to
be most significantly impacted by public health initiatives that aim to lower
the incidence of preeclampsia, hemorrhage, and sepsis.
Other causes were minimal.