1. Baseline Examination Findings
Physical examination of the patient revealed bilateral lower limb edema, with a blood pressure of 120/82 mmHg, heart rate of 70 beats per minute, height of 181 cm, weight of 97 kg, and a body mass index (BMI) of 29.61 kg/m². Laboratory tests (Table 1) showed the following results: renal function indicators included blood urea nitrogen 10.37 mmol/L, creatinine 186.84 μmol/L, uric acid 598.43 μmol/L, and estimated glomerular filtration rate (eGFR) 35.99 mL/min/1.73m²; 24-hour urinary protein quantification was 2.1 g/24h, and urinalysis indicated 2+ urinary protein and 0-3 red blood cells per high-power field (HP) under microscope; serum IgA was 4.02 g/L; hepatitis B virus core antibody (HBcAb) and surface antibody (HBsAb) were positive, while other hepatitis B virus markers and hepatitis B DNA were negative. Renal ultrasonography showed that both kidneys had normal size and morphology, accompanied by enhanced cortical echogenicity and indistinct corticomedullary differentiation.
Table 1 Admission hematology test data
Parameter | Value (reference range) |
Hematology | |
White blood cell count, 109/L | 5.63(3.50-9.50) |
Hemoglobin, g/L | 136(130-175) |
Platelet count, 109/L | 164(125-350) |
Blood chemistry | |
Total protein, g/L | 75.33(65-85) |
Urea nitrogen, mmol/L | 10.37(3.1-8.0) |
Creatinine, μmol/L | 186.84(57-97) |
eGFR, ml/min/1.73m2 | 35.54(≥90) |
Total cholesterol,mmol/L | 4.72(2.9-5.17) |
Triglyceride,mmol/L | 4.08(0.22-1.7) |
Parathyroid hormone,pg/ml | 79.42(15-65) |
Ca+,mmol/L | 2.36(2.11-2.52) |
IP+,mmol/L | 1.08(0.85-1.51) |
FK506,ng/ml | 2.3 |
ALT, U/L | 22.06(9-50) |
AST, U/L | 20.27(15-40) |
LDH, U/L | 181.87(120-250) |
FBS,mmol/L | 5.31(3.9-6.1) |
infection | |
HBsAb,IU/L | 53.9(0-10) |
HBsAg,IU/L | 0.415(0-1) |
HBcAb,IU/L | 0.165(>1) |
HBeAb,IU/L | 1.65(>1) |
HBeAg,IU/L | 0.109(0-1) |
HBV-DNA, IU/ml | <5(0-500) |
Urinalysis | |
protein | 2+ |
Red blood cell, /HPF | 0-1 |
| 0-2 |
| 1-3 |
24h UTP, mg | 2093.50(0-150) |
| 1560.01(0-150) |
| 1625.74(0-150) |
Abbreviations: eGFR, estimated glomerular filtration rate; AST, aspartate aminotransferase;ALT, alanine aminotransferase; LDH, lactate dehydrogenase; FBS, fasting blood sugar; Ig, immunoglobulin; PLA2R, phospholipase A2 receptor;MPO, myeloperoxidase; PR3, proteinase 3; ANCA, anti-neutrophil cytoplasmic antibody;UTP, urine Total Protein.
2. Renal Biopsy Pathological Results
Light microscopiy of the renal biopsy reveals(Figure 1): partial glomerular ischemic sclerosis, mild expansion of the mesangial area, and proliferation of mesangial cells with an increase in mesangial matrix. Uneven renal tubular tissue damage, observable interstitial fibrosis and tubular atrophy, focal arteriolar hyaline degeneration, thickening of interlobular arterial intima, luminal narrowing, and even occlusion. No acute pathological changes, such as crescents or collateral necrosis, were observed. Immunofluorescence showed (Figure 2) IgA(4+), IgM(3+), C3(2~3+), light chain Kappa(2+), Lambda(4+), presenting diffuse, spherical, or clustered deposits in the mesangial area. IgG, IgG1, IgG2, IgG3, IgG4, PLA2R, C1q, C4 were negative(Table 2). Immunohistochemical staining showed that HBsAg and HBcAg were negative. Electron Microscopy Examination (Figure 1) demonstrated an increase in glomerular volume. The mesangial matrix was slightly increased, with a large number of clustered electron-dense deposits in the mesangial area. Diffuse deposition of a small amount of clumped electron-dense deposits was seen in the subendothelium and subsegmental epithelium. The glomerular basement membrane showed segmental thickening (440-1300 nanometers) in areas without deposits. Local swelling of capillary endothelial cells was noted. The pathological features were consistent with IgAN (M0E0S0T2C0).
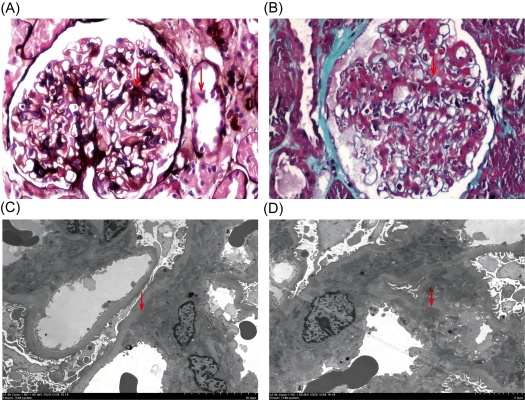
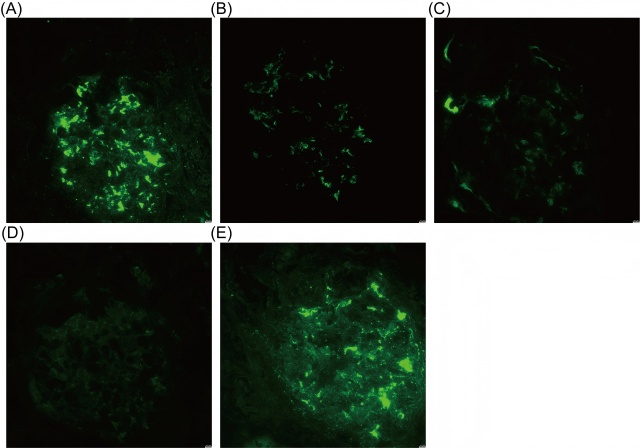
Table 2 Immunization-related examination data for admission
Parameter | Value (reference range) |
IgG, g/L | 12(7-16) |
IgM, g/L | 0.94(0.4-2.3) |
IgA, g/L | 4.02(0.7-4.0) |
C3, g/L | 1.280(0.9-1.8) |
C4, g/L | 0.350(0.1-0.4) |
PLA2R, RU/ml | 0.99(0-20) |
anti-dsDNA, U/mL | 5.14(0-16) |
Antinuclear antibodies | normal |
pANCA | normal |
cANCA | normal |
MPO, RU/ml | 1.06(0-20) |
PR3, RU/ml | 3.14(0-20) |
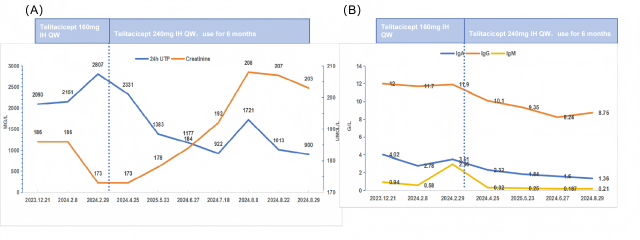
3. Treatment Outcomes
After determining the renal pathology, the patient initiated treatment with Telitacicept at a dosage of 160 mg per week and entecavir antiviral therapy. After 2 months of treatment, the 24-hour urinary protein excretion was reassessed at 2.81 g, and serum creatinine was 173μmol/L. Given the lack of significant improvement in proteinuria and considering the patient's relatively high baseline body weight (BMI 29.61 kg/m²), the dose of Telitacicept was adjusted to 240 mg per week. After 7 months of treatment, the 24-hour urinary protein excretion was reassessed at 0.90 g, serum creatinine was 203μmol/L, IgA was 1.36g/L, IgM <0.21g/L, and IgG was 8.75g/L. Meanwhile, the patient's ALT was 34.17 U/L, AST was 42.74 U/L, and LDH was 232.56 U/L, and no significant liver injury was seen. The patient achieved clinical partial remission without the occurrence of adverse events such as infection or hepatic injury. Changes in the main indicators during the patients' treatment follow-up are shown in Figures 3.