Of 60 studies; 28 reported determinants (4 explicit, 24 implicit): North America (NA) 16, Australia/New Zealand (ANZ) 4, United Kingdom (UK)/Ireland 3, and Europe (EU) 5.
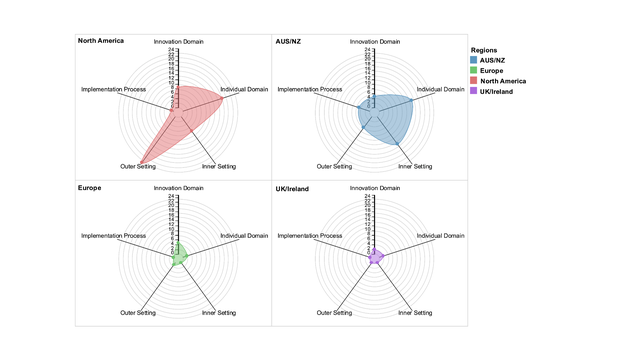
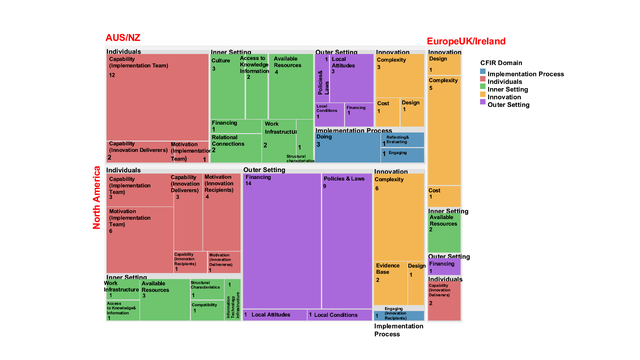
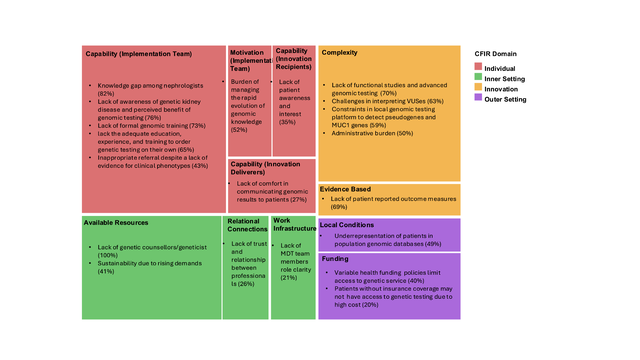
Barriers: NA: individual (18) and outer setting (29) predominated, notably limited implementation team capability/motivation (13), low care recipients capability/motivation (5), financing constraints (14), and insurer pre-authorization requirement (9). ANZ: individual (15) and inner setting (15) predominated with lack of available resources (4), culture (3), infrastructure (3), limited access to knowledge (2), weak relational connections (2), and financing gap (1). Reporting from UK/EU was limited: innovation (7) with service complexity (5) reported most often. Domain-stratified barriers across regions are shown in Fig 1-2.
51 survey responses corroborated the review patterns (Fig 3).
Top barriers in descending orders: implementation team capability (22), financing (16), innovation complexity (14), policies/laws (10), available resources (9), and team motivation (8).
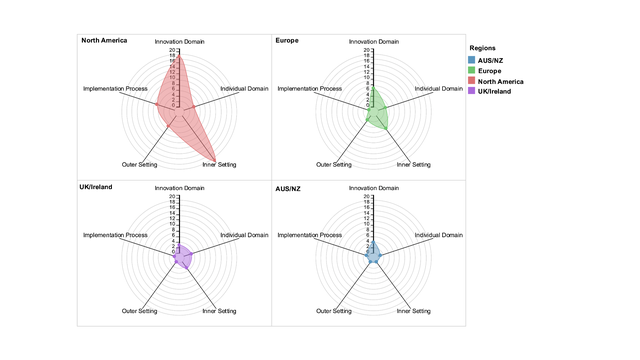
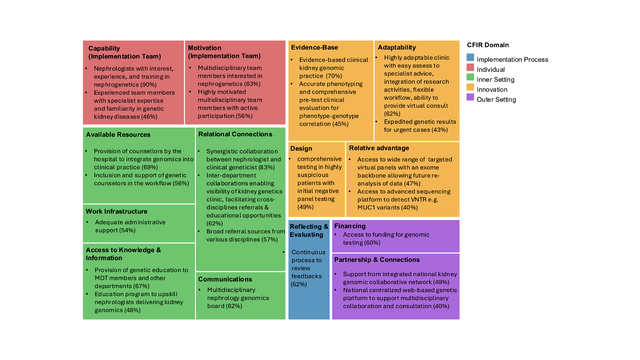
Facilitators: Across regions, innovation (33) and inner setting (30) predominated. Within innovation, relative advantage (12), design quality (12), adaptability (7), and evidence-base (2) supported implementation. Within inner setting, strong relational connections (14), available resources (8), access to knowledge/information (3), and genetics-centered culture (2) enabled implementation.
Domain-stratified facilitators are shown in Fig 4-5; survey responses mirrored the review findings (Fig 6).
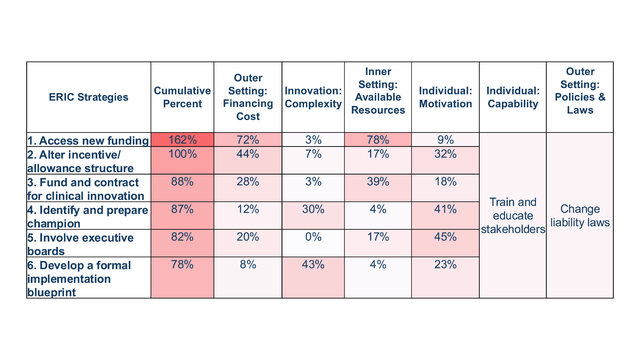
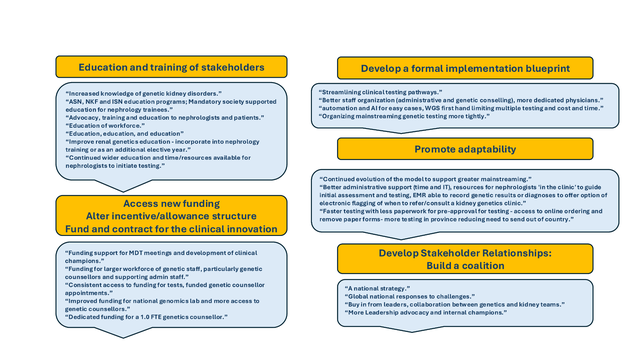
Strategies: Top matched strategies using ERIC tool in descending orders: train/educate stakeholders, change liability laws, secure funding 162%, alter incentive structure 100%, fund clinical innovation 88%, identify and prepare champions 87%, involve executive boards 82%, develop a formal implementation blueprint 78% (Fig 7). Strategies proposed by global leads mimicked ERIC-derived priorities (Fig 8).